

Introduction
The transcutaneous (external skin) approach for placing or revising jaw angle implants—implants positioned at the mandibular angle—is a recognized technique in aesthetic and reconstructive facial surgery. Unlike the more common intraoral (inside-the-mouth) approach, the transcutaneous method provides direct external access to the mandibular angle, offering certain technical and clinical advantages in selected cases.
Indications
The external approach may be indicated when one or more of the following conditions apply:
-
Revision surgery following a previous intraoral jaw angle implant that is malpositioned (especially if positioned too high) or complicated by infection, making intraoral re-entry less desirable.
-
Need for improved visualization and direct access at the implant–bone interface, particularly when vertical lowering or screw fixation is required.
-
Patient preference, such as avoidance of intraoral incisions, concern about infection, or prior intraoral surgery that compromised tissue quality or healing.
-
Male patients with beard-bearing skin, where a small external incision can heal well with minimal scarring.
-
Overlay or augmentation procedures, such as placing additional implants over existing custom jawline implants when intraoral access is inadequate.
The success of the external jaw angle approach depends on careful incision placement. The incision is typically located directly over or just posterior to the mandibular angle—often within the beard region in male patients or within a natural skin crease—to minimize visible scarring. This location also avoids the marginal mandibular branch of the facial nerve, in contrast to lower neck incisions.
Case Study
![]()
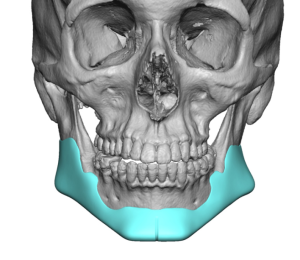
 A male patient presented following removal of a prior custom jawline implant due to chronic infection. After six months of healing, he elected to undergo placement of a new custom jawline implant while avoiding intraoral incisions to reduce reinfection risk. He expressed no concern regarding potential external scars.
A male patient presented following removal of a prior custom jawline implant due to chronic infection. After six months of healing, he elected to undergo placement of a new custom jawline implant while avoiding intraoral incisions to reduce reinfection risk. He expressed no concern regarding potential external scars.


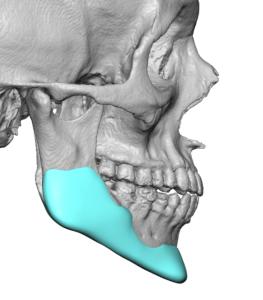
![]() Through the original submental incision and new direct jaw angle incisions, a continuous subperiosteal pocket was developed along the jawline. The custom jawline implant was introduced from front to back and secured with screws at each incision site. To enhance jaw angle width, standard jaw angle implants were placed as onlays over the angle portions of the custom implant.
Through the original submental incision and new direct jaw angle incisions, a continuous subperiosteal pocket was developed along the jawline. The custom jawline implant was introduced from front to back and secured with screws at each incision site. To enhance jaw angle width, standard jaw angle implants were placed as onlays over the angle portions of the custom implant.

 The wounds were closed in multiple layers using small resorbable sutures. The patient healed uneventfully, and the long-term external scars were inconspicuous and of no concern to him.
The wounds were closed in multiple layers using small resorbable sutures. The patient healed uneventfully, and the long-term external scars were inconspicuous and of no concern to him.
Discussion
Although not the primary access method for jaw angle implant placement in aesthetic facial surgery, the transcutaneous approach offers distinct advantages when appropriately indicated:
Advantages
-
Superior visualization of the implant–bone interface, enabling precise placement, alignment, repositioning, and screw fixation.
-
Reduced risk of contamination and infection compared to intraoral access.
-
Avoidance of reopening prior intraoral incisions, which may harbor scar tissue or exhibit compromised healing.
-
Minimal scarring when incisions are placed in favorable skin regions, such as beard-bearing areas in men.
Disadvantages and Risks
-
Presence of an external incision, with potential for a visible scar (though often minimal when well positioned).
-
Risk of injury to the marginal mandibular branch of the facial nerve if dissection is not performed carefully.
-
Limited access due to smaller incision size.
-
Technical difficulty when inserting large or rigid implants through a small external tunnel.
Patient Selection
Ideal candidates include male patients undergoing revision jaw angle implant surgery where intraoral access is problematic and who are willing to accept a small, potentially well-camouflaged scar in exchange for improved implant accuracy and reduced infection risk. The approach should be avoided in patients who are highly scar-averse, have thin soft-tissue coverage at the jaw angle (risking implant visibility or palpability), or require placement of large, rigid implants not suitable for small external access.
Conclusion
The transcutaneous (external) approach to jaw angle implant placement is a valuable adjunctive technique, particularly in revision cases or when intraoral access is undesirable. It offers improved visualization and lower infection risk at the expense of a small, external incision with minimal scar potential when properly executed.
Key Points
-
Jaw angle and jawline implants are traditionally placed through intraoral posterior vestibular incisions.
-
The external approach is most often employed secondarily, typically after implant removal due to infection.
-
Scars from direct external jaw angle incisions generally heal well in the male beard area.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon