

Breast augmentation in transfeminine (transfemales / trans women) patients is a well-established procedure, but it has some important differences from augmentation in cisgender women due to anatomical and hormonal factors.
1. Background: Hormone Therapy First
Most transfeminine patients undergo estrogen-based hormone therapy before considering surgery. This:
- Promotes natural breast development (often A–small B cup)
- Helps shape the chest tissue and skin envelope
However, hormone-induced growth is often limited, which is why many pursue augmentation.
2. Key Anatomical Considerations
![]()
Compared to cisgender women, transfeminine patients often have:
- Wider chest wall
- Less native breast tissue
- Larger nipple–areola complex (sometimes)
- More laterally positioned nipples
- Thicker pectoralis muscle
These factors can influence implant selection and placement.
3. Implant Selection
Surgeons typically consider:
- Larger implant volumes (to match chest width and achieve proportional cleavage)
- Wider base diameter implants
- Silicone implants are most commonly used for a more natural feel
High-profile implants are often chosen to enhance projection when tissue is limited.
4. Implant Placement
Options:
- Subglandular (above muscle)
- Better cleavage
- Less animation deformity
- Requires enough soft tissue coverage
- Submuscular (dual-plane)
- More natural slope in thin patients
- Better implant camouflage when tissue is minimal
Choice depends on tissue thickness and aesthetic goals.
5. Incision Options
- Inframammary fold (most common) – best control and precision
- Periareolar – less common due to limited areolar size
- Transaxillary – possible but less commonly used
6. Aesthetic Goals
Common goals in transfeminine patients:
- Creation of cleavage which is not always possible
- Feminine breast contour
- Proper medial positioning (often more challenging due to wider sternum)
7. Outcomes and Satisfaction
- High satisfaction rates overall
- Significant improvement in gender dysphoria and body image
- Results can be very natural when planned appropriately
8. Risks and Considerations
Same general risks as any breast augmentation:
- Capsular contracture
- Implant malposition (higher risk of lateral displacement in wider chests)
- Need for revision surgery
- Sensation changes
9. Timing
- Typically recommended after 12–24 months of hormone therapy
- Ensures maximum natural development before surgery
Case Example
![]() This small petite transfemale desired a combination of breast augmentation and rib removal surgeries. She had been on hormone therapy for years and had developed a small amount of breast tissue that had remained stable. her
This small petite transfemale desired a combination of breast augmentation and rib removal surgeries. She had been on hormone therapy for years and had developed a small amount of breast tissue that had remained stable. her
goal was a fuller ‘B cup’.
![]()
![]() After the completion of rib removal surgery in the prone position she moved to the supine position where 200cc moderate plus silicone implants were placed through 1” transaxillary incisions in the dual plane pocket.
After the completion of rib removal surgery in the prone position she moved to the supine position where 200cc moderate plus silicone implants were placed through 1” transaxillary incisions in the dual plane pocket.

![]() What is important to appreciate, even though this is an jntraop result with the patient laying in the supine position which is not necessarily how the implants will look in the vertical upright position, that small implants are not going to create cleavage, decrease the wide sternal gapappearance, or correct existing nipple-areolar asymmetries.
What is important to appreciate, even though this is an jntraop result with the patient laying in the supine position which is not necessarily how the implants will look in the vertical upright position, that small implants are not going to create cleavage, decrease the wide sternal gapappearance, or correct existing nipple-areolar asymmetries.
Discussion
Implant sizing in transfeminine patients is less about “cup size” and more about matching implant dimensions to chest anatomy—this is where it differs most from cisgender augmentation.
Here are the key strategy principles I use:
1. Base Width Is the Starting Point (Most Important)
The breast base diameter (BWD) determines the maximum implant width.
In transfeminine patients:
- Chest walls are typically wider
- Nipples are often more lateral
?? Strategy:
- Choose an implant with a wide base diameter to match the chest
- Avoid implants that are too narrow ? leads to:
- Wide cleavage gap
- “Separated” breast appearance
Key point:
If you undersize the width, no amount of projection will fix poor cleavage.
2. Volume Is Usually Higher Than Expected
Because of:
- Wider chest
- Less native tissue
- Desire for visible cleavage
?? Typical ranges:
- For significant augmentation 350–600+ cc, sometimes larger depending on frame
- For modest augmentations in smaller patients 150-200ccs may be enough
But volume alone is misleading—width + projection matters more than cc number.
3. Profile Selection (Critical Tradeoff)
Profile determines how much the implant projects relative to its width.
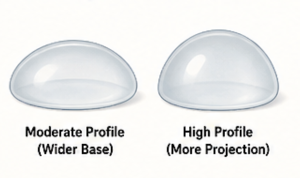
Moderate Profile
- Wider base, less projection
- Better chest matching
- Can look flatter in low-tissue patients
High / Extra-High Profile
- Narrower base, more projection
- Helps create anterior fullness
- Useful when:
- Soft tissue is limited
- Need to “push” cleavage forward
?? Common strategy in transfeminine patients:
- High profile implants with relatively large volume in patients that want a larger breast augmentation result
- Lower profiles and smaller volumes are better in the patient who wants to stay in the smaller B cup size
- Balance projection + chest width
4. Cleavage Strategy (A Major Challenge)
![]()
Due to:
- Wider sternum
- Laterally positioned nipples
Natural cleavage is hard to achieve
Techniques:
- Select implants with maximum medial width
- Consider slight over-dissection medially (with caution)
- Use larger implants to help fill the medial space
Limitation:
- True cleavage may not be achievable anatomically
- In smaller implant sizes cleavage will not be achieved
5. Soft Tissue Thickness Assessment
Pinch test at upper pole:
- >2 cm thickness
Can consider subglandular placement - <2 cm thickness
Dual-plane/submuscular preferred for camouflage
Sizing implication:
- Thin patients often need:
- More projection
- Possibly slightly smaller width to avoid edge visibility
6. Nipple Position Drives Centering
Implants should be centered under the nipple—but:
- Nipples may be lateral
- Chest is wide
?Options:
- Accept slightly lateral breast position (most common)
- Or adjust pocket medially (limited by anatomy)
This directly affects perceived size and cleavage.
7. Skin Envelope & Expansion
Transfeminine patients often have:
- Tight lower pole
- Limited ptosis
Strategy:
- Implants may be used to expand the lower pole
- Slightly larger implants help shape the breast footprint
8. Sizers and 3D Planning
More critical in this population:
- External sizers help visualize proportion on a wider chest
- 3D imaging may help simulate:
- Cleavage
- Lateral fullness
- Projection
9. Avoiding Common Sizing Mistakes
Frequent pitfalls:
- Choosing implants based on “cup size”
- Using too narrow implants ? wide cleavage gap
- Underestimating needed volume
- Ignoring chest width
- Over-aggressive medial dissection ? symmastia risk
10. Practical Sizing Algorithm (Simplified)
- Measure base width (cm)
- Choose implant with matching or slightly smaller width
- Decide profile:
-
- Thin tissue – higher profile
- Thicker tissue – moderate/high
- Select volume that:
-
- Fills width
- Achieves desired projection
- Confirm with sizers / simulation
- But in the end patient tolerance for change will dictate implant size
Dr Barry Eppley
Plastic Surgeon