

Correction/repositioning of sagging brows is done by well known browlift procedures. The vast majority of browlift surgeries are done in women with access to do the procedure coming from above in and behind the frontal hairline. The three different female browlift techniques (coronal, pretrichial and endoscopic) are chosen based on forehead skin length and the position of the frontal hairline.
Browlifts in men, however, are more challenging because of the typical lack of a stable hairline, poor hair density or no hairline at all. Thus, most men can not have a superior scalp approach due to concerns of visible scarring or disturbed hairline concerns. Browlifts in many men have more limited options and include either a mid-forehead, direct (superior eyebrow hairline) or a transpalpebral incisional approaches.
 The transpalpebral browlift technique is used almost exclusively in men and relies upon a device (Endotine) to achieve the browlifting effect. In addition it has a browlifting effect that is largely limited to the outer half of the brow (temporal brow) and creates a more modest lifting effect. This location of the browlift is what makes it most useful in men as inner browlifting creates an unnatural appearance for most men.
The transpalpebral browlift technique is used almost exclusively in men and relies upon a device (Endotine) to achieve the browlifting effect. In addition it has a browlifting effect that is largely limited to the outer half of the brow (temporal brow) and creates a more modest lifting effect. This location of the browlift is what makes it most useful in men as inner browlifting creates an unnatural appearance for most men.
 The transpalpebral browlift is done from an upper blepharoplasty incision and is often done in conjunction with removal of upper eyelid skin. After the upper eyelid skin is removed, the outer brow bone is accessed in a subperiosteal fashion. Dissection is carried above the lower edge of the outer brow bone in excess of 15mms to allow the Endotine device to fit.
The transpalpebral browlift is done from an upper blepharoplasty incision and is often done in conjunction with removal of upper eyelid skin. After the upper eyelid skin is removed, the outer brow bone is accessed in a subperiosteal fashion. Dissection is carried above the lower edge of the outer brow bone in excess of 15mms to allow the Endotine device to fit.
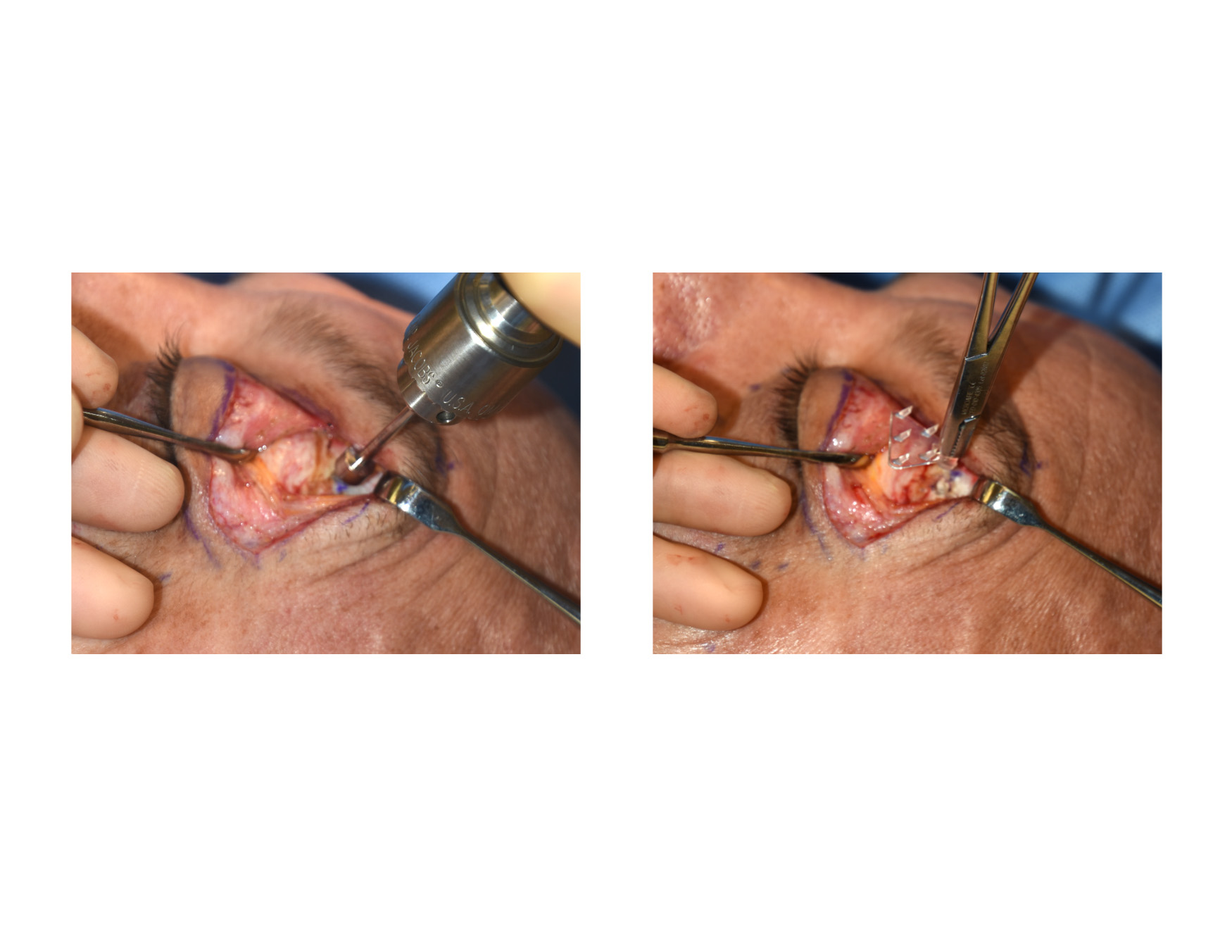 At 15mms above the lower edge of the brow bone an outer cortical bone is drilled. This allows the Endotine device to be inserted into the hole and oriented in an upright triangular position. This allows the prongs on the device to be angled upward.
At 15mms above the lower edge of the brow bone an outer cortical bone is drilled. This allows the Endotine device to be inserted into the hole and oriented in an upright triangular position. This allows the prongs on the device to be angled upward.
 Once the Endotine device is inserted, the outer brow tissues are lifted and suspended on the device’s prongs. The soft tissue are then closed over the device and the upper blepharoplasty incision closed.
Once the Endotine device is inserted, the outer brow tissues are lifted and suspended on the device’s prongs. The soft tissue are then closed over the device and the upper blepharoplasty incision closed.
The transpalpebral browlift is essentially a ‘push’ browlift from below. This is stark contrast to the more traditional browlift methods which are ‘pull’ procedures from above. The Endotine device makes this possible. It is composed of a resorbable polymer material which breaks down and is absorbed completely within 6 to 9 months after it is inserted. This should be enough time to allows the brow lift tissues to scar down and heal to the bone in a slightly more elevated position.
Patients will feel the device under the skin for a few months after the procedure although it is not visible on the outside. For men the transpalpebral approach, while having a modest result, avoids scar concerns at the eyebrow or on the forehead which can take a long time to mature and their imperceptibility is not always assured.
Dr. Barry Eppley
Indianapolis, Indiana