

Waistline narrowing by rib removal is almost an urban myth. There is a lot of internet chatter and interest in the procedure but it is hard to actually find a surgeon who does it or a patient who has had it. In reality, it is a plastic surgery procedure that is done but only by those few surgeons who feel comfortable working around the rib structures and can do it with small incisions and a low risk of any serious complications. (e.g., pneumothorax)
Typically the ribs removed for waistline narrowing have been described as that of the free floating 11th and 12th ribs. This is done through a small incision in the back. While these are the ‘easiest’ ribs to remove because they are well below the lowest level of the pleura, they often are not enough to get the best waistline narrowing result. I prefer to also remove rib 10 or do an intermediate resection of it (so that the distal end will naturally move inward without a posterior attachment) to get maximal waistline narrowing. The addition of rib #10 removal can make a dramatic difference as this rib turns the corner around the waistline much more so than the free floating ribs below it.
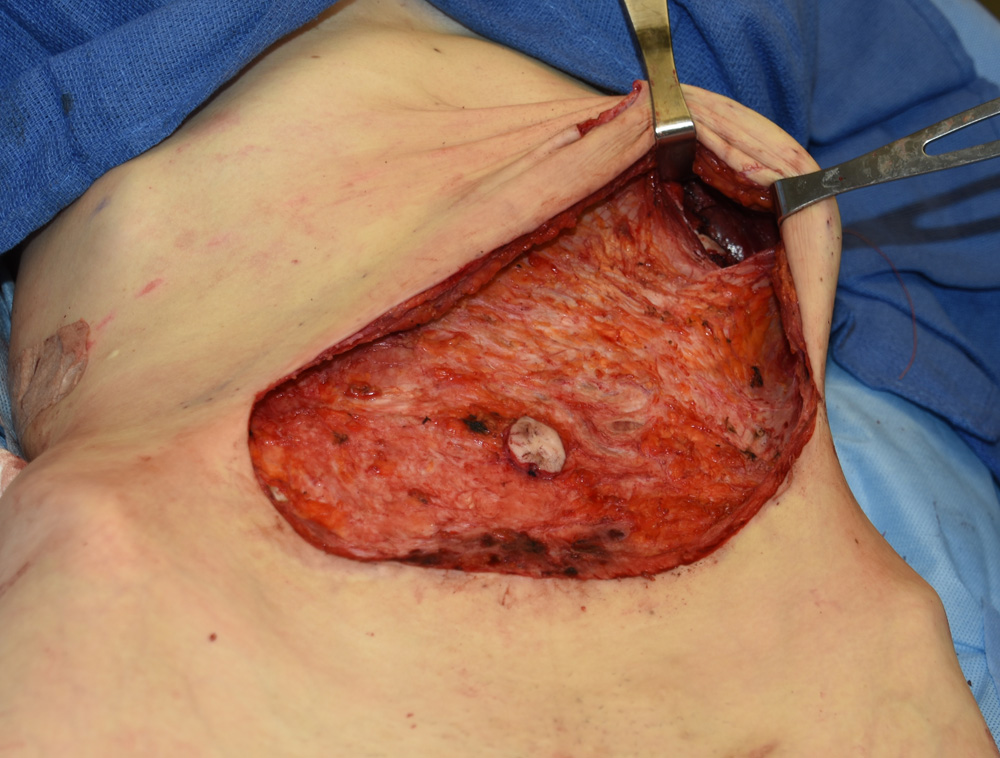
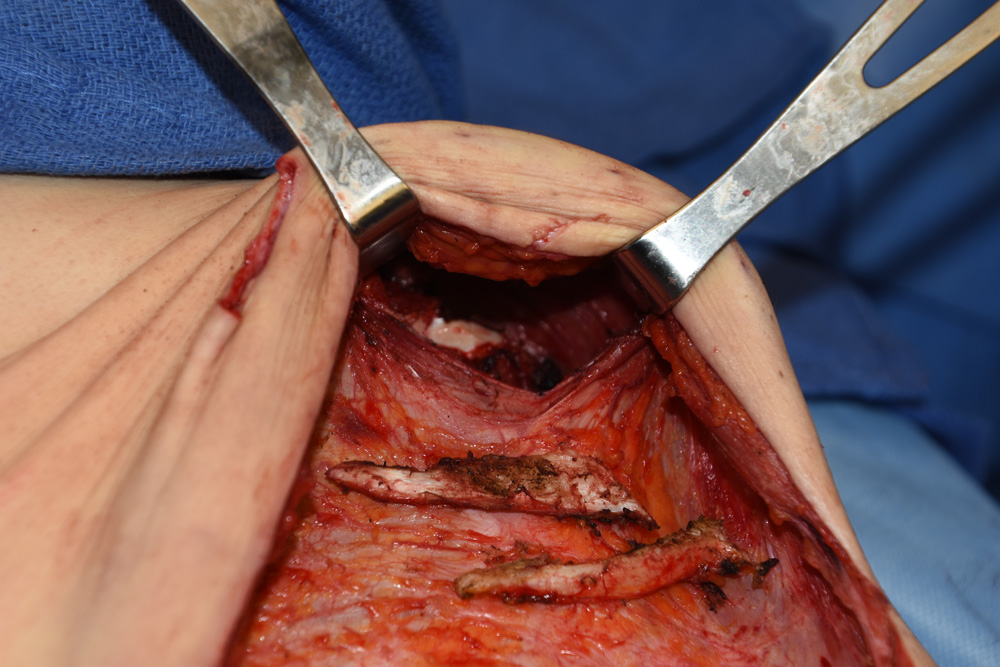 Rib removal can also be done through a tummy tuck approach. But this is for a different torso effect. The ribs removed through a tummy tuck are #8 and #9 ribs. This is done by splitting the rectus muscle vertically which allows access to the subcostal area. Ribs # 8 and 9 are easily removed but they will not have a waistline narrowing effect per se as they lie above the anatomic waist. They may help to vertically lengthen the torso but their anterior position prevents from creating a true inward waistline effect.They are removed to reduce a subcostal prominence or protrusion.
Rib removal can also be done through a tummy tuck approach. But this is for a different torso effect. The ribs removed through a tummy tuck are #8 and #9 ribs. This is done by splitting the rectus muscle vertically which allows access to the subcostal area. Ribs # 8 and 9 are easily removed but they will not have a waistline narrowing effect per se as they lie above the anatomic waist. They may help to vertically lengthen the torso but their anterior position prevents from creating a true inward waistline effect.They are removed to reduce a subcostal prominence or protrusion.
While it seems like a long way from a low abdominal incision (and it is), the subcostal margin is well within reach. It does require a full length tummy tuck to do so however. It is best and less uncomfortable for patients after surgery to vertically split the rectus muscle rather than transecting it horizontally. The intraoperative injection of Exparel into the muscle as well as an intercostal block goes a long way with managing postoperative discomfort with this surgery.
Dr. Barry Eppley
Indianapolis, Indiana