

A tummy tuck is a major abdominal operation that usually removes a large horizontal ellipse of lower abdominal skin and fat. While tremendously effective, many patients having the procedure have excess fat beyond the zone of the tummy tuck excision whose reduction would improve the overall abdominal contouring result. While liposuction of the flanks is commonly done with a tummy tuck, liposuction of the abdominal area above the cut out has been frowned upon because of concerns of impairing healing of the tummy tuck excision.
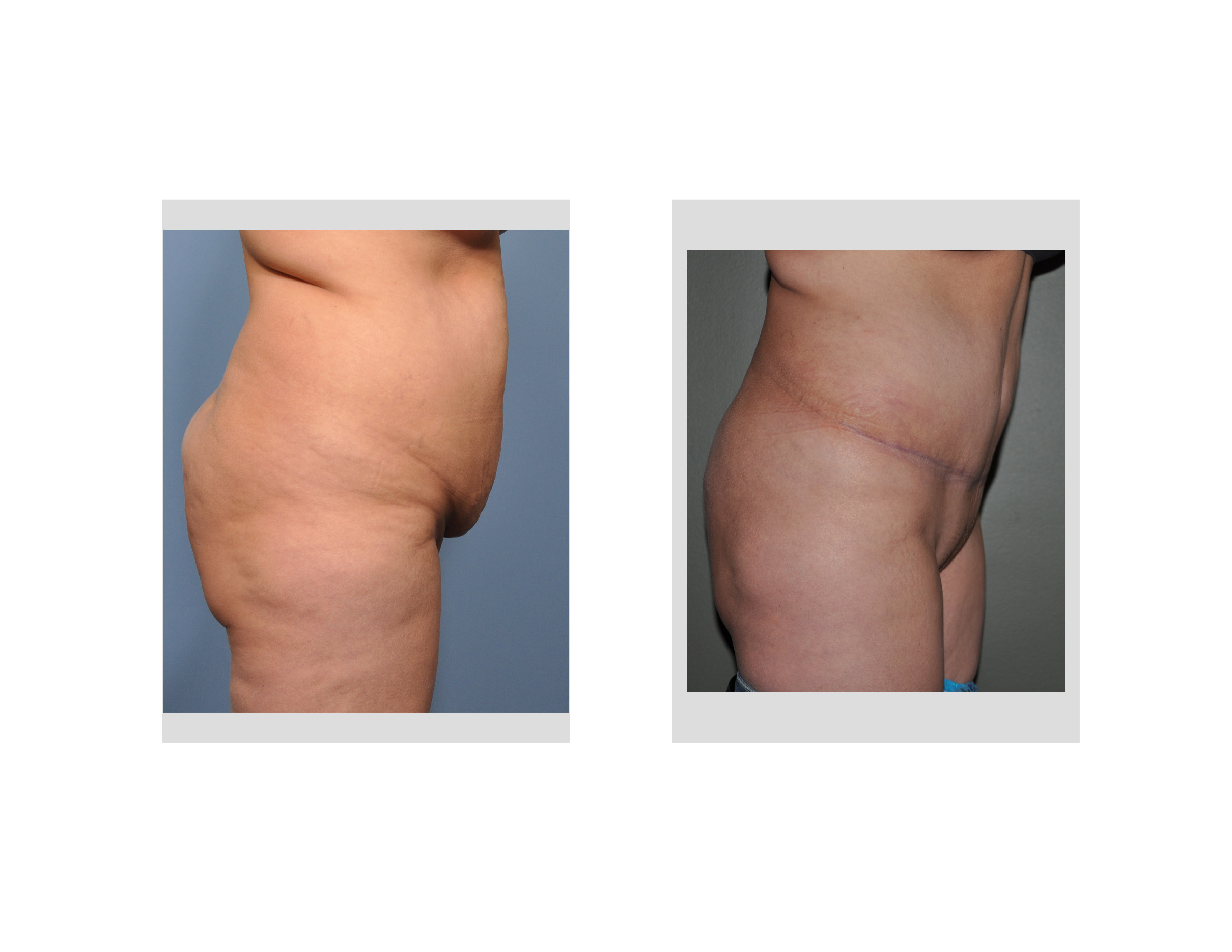
 Avoidance of any upper abdominal liposuction at the time of a tummy tuck is certainly the safest approach as there is no chance of vascular compromise by not doing so. But this can leave an upper abdominal fullness that protrudes out beyond the more inwardly located tummy tuck scar the entire lower abdominal area. Many patients interpret this postoperative finding as swelling only to discover it never goes away. This is due to a simple anatomic fact the thickness of the upper abdominal fat largely remains the same while the lower abdominal contour is better because a large segment of tissue has been removed.
Avoidance of any upper abdominal liposuction at the time of a tummy tuck is certainly the safest approach as there is no chance of vascular compromise by not doing so. But this can leave an upper abdominal fullness that protrudes out beyond the more inwardly located tummy tuck scar the entire lower abdominal area. Many patients interpret this postoperative finding as swelling only to discover it never goes away. This is due to a simple anatomic fact the thickness of the upper abdominal fat largely remains the same while the lower abdominal contour is better because a large segment of tissue has been removed.
In the May 2015 issue of the journal Plastic and Reconstructive Surgery, an article appeared in print entitled ‘Safely Combining Abdominoplasty with Aggressive Abdominal Liposuction Based on Perforator Vessels: Technique and a Review of 300 Cases’. A retrospective review of 300 consecutive patients who had a tummy tuck combined with liposuction. The tummy tuck was performed saving several perforators from the deep superior epigastric artery. The abdominal liposuction was fairly aggressive removing an average of 660cc. Their overall complication rate was 17% (52 patients) of which the vast majority of the patients suffered minor complications (the need for scar revision, seroma evacuations, and non-surgical treatment of incisional dehiscences being the most common) and 1% encountered major complications. (non-fatal pulmonary embolus, severe infection and need for blood transfusion)
 Combining extensive liposuction with a tummy tuck has been a somewhat controversial combination since the early 2000s. What has changed since then is a better appreciation of the blood supply to the abdomen. This study uses a tummy tuck technique that preserves perforator vessels to the central abdominal skin flap. This then permits the central abdominal area to safely undergo liposuction with impairing perfusion to the central abdominal skin above the incision line.
Combining extensive liposuction with a tummy tuck has been a somewhat controversial combination since the early 2000s. What has changed since then is a better appreciation of the blood supply to the abdomen. This study uses a tummy tuck technique that preserves perforator vessels to the central abdominal skin flap. This then permits the central abdominal area to safely undergo liposuction with impairing perfusion to the central abdominal skin above the incision line.
In the standard lipoabdominoplasty technique the liposuction is performed first followed by the tummy tuck. The liposuction loosens up enough of the upper abdominal tissues that extensive abdominal flap undermining is not needed and all perforators are preserved. This tummy tuck technique performs the liposuction after the tummy tuck. The difference is that some upper abdominal flap undermining is done and the perforators are deliberately seen and preserved.
Dr. Barry Eppley
Indianapolis, Indiana