


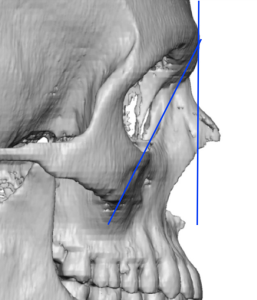
 Common aesthetic deformities of the lower eyelid include tear troughs, undereye hollows and orbitomalat grooves. While these all occur from age-related periorbital changes due to soft tissue atrophy and tissue laxity, when they are seen in young patients they are more likely a function of a bony deficiency. Specifically an infraorbital-malar deficiency the extent of which depends on whether a negative orbital vector is present (a clinical measurement) or an increased brow to infraorbital rim angle exists.
Common aesthetic deformities of the lower eyelid include tear troughs, undereye hollows and orbitomalat grooves. While these all occur from age-related periorbital changes due to soft tissue atrophy and tissue laxity, when they are seen in young patients they are more likely a function of a bony deficiency. Specifically an infraorbital-malar deficiency the extent of which depends on whether a negative orbital vector is present (a clinical measurement) or an increased brow to infraorbital rim angle exists.
Surgical augmentation of the infraorbital rim can be done by either standard or custom infraorbital rim implants each of which has their specific indications. Differences in their implant footprint create different dimensional effects. One of their key differences is whether vertical augmentation of the infraorbital rim occurs and to what extent is a malar augmentation effect is achieved.

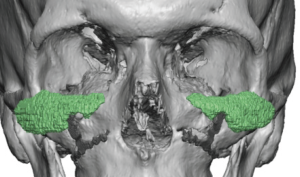
 Standard infraorbital rim implants have their origins in treating age-related rim changes which is why they are historically known as tear trough implants. Their original sizes were small as the tear trough area is just a part of the infraorbital rim. They are probably more commonly used today in younger patients for undereye hollows which is why the extended tear trough or standard infraorbital-malar implant is used. It primarily provides horizontal augmentation along the infraorbital rim and anterior cheek area, it can not create any true vertical augmentation even if pushed high as high along the edge of the rim as it can be secured. As a result it provides 2D infraorbital rim augmentation.
Standard infraorbital rim implants have their origins in treating age-related rim changes which is why they are historically known as tear trough implants. Their original sizes were small as the tear trough area is just a part of the infraorbital rim. They are probably more commonly used today in younger patients for undereye hollows which is why the extended tear trough or standard infraorbital-malar implant is used. It primarily provides horizontal augmentation along the infraorbital rim and anterior cheek area, it can not create any true vertical augmentation even if pushed high as high along the edge of the rim as it can be secured. As a result it provides 2D infraorbital rim augmentation.

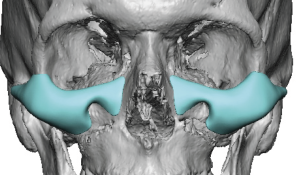
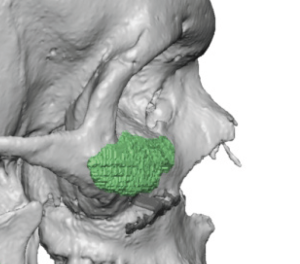
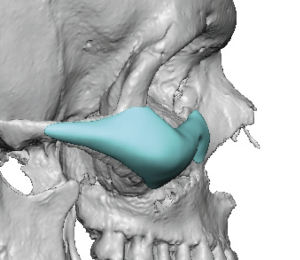 Conversely a custom infraorbital rim-malar implant provides a 3D effect. Not only is the implant footprint extend around the corner of the cheekbone back along the zygomatic arch if desired but it also saddles the in infraorbital rim. This really has an expansion effect on the entire bony complex around the eye rather than the spot augmentation of a smaller section of the infraorbital rim that tear trough implants achieve.
Conversely a custom infraorbital rim-malar implant provides a 3D effect. Not only is the implant footprint extend around the corner of the cheekbone back along the zygomatic arch if desired but it also saddles the in infraorbital rim. This really has an expansion effect on the entire bony complex around the eye rather than the spot augmentation of a smaller section of the infraorbital rim that tear trough implants achieve.
When to use these various forms of infraorbital implants depends on the problem being treated. From my experience the key indicator is that of the lower eyelid. If the lower eyelid has a good position without rounding or sag then standard infraorbital rim implants will probably suffice. Even if a slight sag is present standard implants will work as long as there is no malar or cheek flattening/deficiency. But when a negative orbital vector its present, significant lid sag exists and the cheeks are flat only a custom infraorbital-malar implant approach more completely treats the scope of the problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon