

The side of the head represents two of the five visible surfaces of the skull, so it’s no surprise that its shape can become an aesthetic concern. These concerns typically relate to the width of the sides of the head, which can appear either too narrow or too wide.
When the sides of the head are too narrow, the overall skull shape is often constricted as well, indicating an underlying bony deficiency. In such cases, the only effective solution is skull bone augmentation.
Conversely, when the sides of the head are too wide or convex, the problem often lies in the soft tissue — particularly a thick temporal muscle — rather than the bone.
Why Anatomy Matters
 For those with an overly wide or convex head shape, understanding the musculoskeletal anatomy of the temporal region is key. Unlike the front, top, and back of the head, the sides have substantial muscle coverage, whose thickness depends on the contour of the underlying temporal bone.
For those with an overly wide or convex head shape, understanding the musculoskeletal anatomy of the temporal region is key. Unlike the front, top, and back of the head, the sides have substantial muscle coverage, whose thickness depends on the contour of the underlying temporal bone.
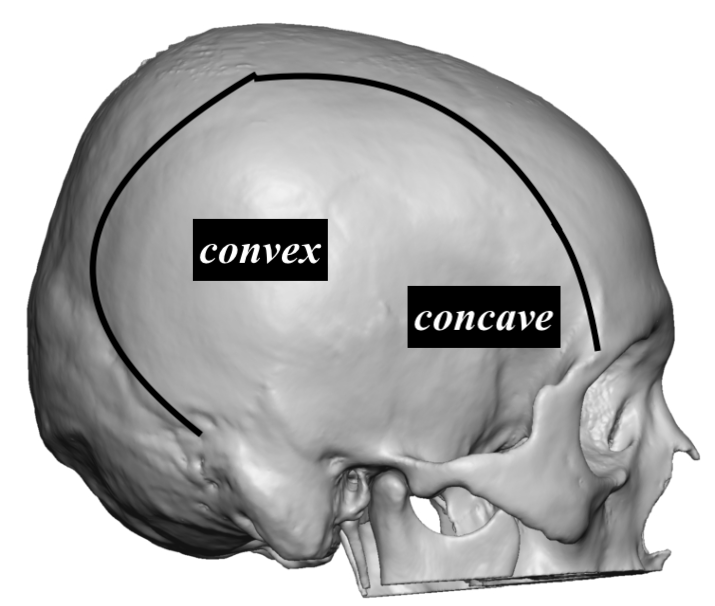
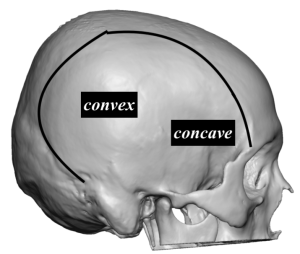
The temporal bone itself has two distinct parts:
-
A concave portion near the eye, known as the temporal fossa,
-
And a convex portion located posteriorly.
The temporal muscle overlays this bone, with its thickness varying accordingly. Approximately 70% of the muscle mass is concentrated over the concave fossa, while it thins out as it extends over the convex portion. Importantly, the muscle originates along the temporal line, where the temporal bone meets the side of the forehead, the top, and the back of the head.
How Temporal Reduction Works
The anatomy of the temporal region provides valuable insight into how temporal reduction surgery is performed, why it is effective, and its limitations.
The goal of the procedure is to reduce the width and convexity of the sides of the head by removing the full thickness of the posterior temporal muscle that lies over the convex bone. While this is not the thickest portion of the muscle, removing approximately 7–10mm per side is usually sufficient to achieve a noticeable improvement.
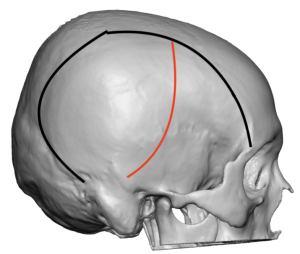 The procedure is performed through an incision hidden behind the ear, following the line where the convex bone transitions into the concave fossa superiorly. (red line) Importantly, removing this segment of muscle has no impact on jaw function and rarely even results in mild stiffness.
The procedure is performed through an incision hidden behind the ear, following the line where the convex bone transitions into the concave fossa superiorly. (red line) Importantly, removing this segment of muscle has no impact on jaw function and rarely even results in mild stiffness.
Limitations
However, the surgery does not extend much into the thicker, anterior portion of the muscle that lies over the concave fossa, due to incision limitations. While most patients do not require treatment in this area, a small degree of residual fullness may sometimes remain. In my experience, this is the primary reason why a sec0ndary procedure might be requested.
Case Study: Long-Term Results and Secondary Reduction
 One male patient underwent temporal reduction surgery with excellent results. Nearly nine years later, he returned requesting a touch-up to address a small area of fullness just above the ears. This area corresponded to the junction between the posterior convex bone and the anterior concave fossa — an area not treated during his initial surgery and not normally is.
One male patient underwent temporal reduction surgery with excellent results. Nearly nine years later, he returned requesting a touch-up to address a small area of fullness just above the ears. This area corresponded to the junction between the posterior convex bone and the anterior concave fossa — an area not treated during his initial surgery and not normally is.
Revision Procedure
-
 Under general anesthesia, a superior postauricular sulcus incision was made.
Under general anesthesia, a superior postauricular sulcus incision was made. -
The deep temporal fascia was opened to expose the muscle.
-
The muscle in the outlined area was carefully dissected from both the overlying fascia and the underlying bone and removed.
-
Remaining visible muscle edges were treated with electrocautery to promote atrophy and create a smooth, feathered contour.
-
The incision was closed with absorbable sutures, and no drains were necessary.
 Under general anesthesia, a superior postauricular sulcus incision was made.
Under general anesthesia, a superior postauricular sulcus incision was made. The deep temporal fascia was opened to expose the muscle.
The deep temporal fascia was opened to expose the muscle. The muscle in the outlined area was carefully dissected from both the overlying fascia and the underlying bone and removed.
The muscle in the outlined area was carefully dissected from both the overlying fascia and the underlying bone and removed. Remaining visible muscle edges were treated with electrocautery to promote atrophy and create a smooth, feathered contour.
Remaining visible muscle edges were treated with electrocautery to promote atrophy and create a smooth, feathered contour. The incision was closed with absorbable sutures, and no drains were necessary.
The incision was closed with absorbable sutures, and no drains were necessary.
 Nearly a decade after his original surgery, his long-term results show a notable improvement in the contour of the sides of his head, as seen in both front and back views.
Nearly a decade after his original surgery, his long-term results show a notable improvement in the contour of the sides of his head, as seen in both front and back views.
Key Takeaways
- Complete posterior muscle removal: Temporal reduction surgery removes the entire posterior portion of the temporal muscle, leaving the larger anterior segment intact.
- Low revision rate: Revisions are uncommon, but when needed, they address a residual bulge at the posterior edge of the anterior muscle, above and in front of the ear.
- Effective revision technique: Through a superior postauricular sulcus incision, this residual fullness can be successfully reduced.
Dr. Barry Eppley
World-Renowned Plastic Surgeon