

Rhinoplasty is one the most challenging and unforgiving operations of all facial plastic surgery operations. Due to the complexity of nasal anatomy and how its multiple parts interrelate, many different surgical maneuvers and changes are possible. Some of these changes are more significant while others are more subtle. But they all can make a difference in the final result, whether it be how the nose looks or how well it breathes.
Because of the importance of the nose to one’s facial appearance and the many different maneuvers that can be done in rhinoplasty, communication between patient and plastic surgeon is absolutely critical. In my Indianapolis plastic surgery practice, I use paper diagrams of the anatomy of the nose during a rhinoplasty consultation and computer imaging forwarded to the patient after the appointment. Both visual methods are essential in having the patient understand what the problems are and what is surgically possible.
In the course of this communication, some appreciation by the patient of the anatomy of the nose and the terms we use in rhinoplasty surgery are necessary to make sure we are really communicating.
Most people underestimate the complexity of the nose because they are thinking only about its visible external appearance. But beneath the skin lies an intricate arrangement of cartilaginous- and bone-based structures that give the nose both its form and function.
 The surface of the nose features a number of distinct regions and structures.
The surface of the nose features a number of distinct regions and structures.
· The root or radix of the nose is the area between and just below the eyebrows. It is the uppermost part of the bridge.
· The bridge lies below the root and forms the upper one-third of the nose.
· The middle vault lies between the bridge and the tip of the nose.
· The dorsum (roofline) is the shape and height of the nose as it runs between the root and the tip of the nose.
· The tip of the nose is where the dorsal line of the nose meets the columella.
· The columella is the strip of skin between the nostrils which extends down from the tip to the upper lip.
· The ala are the sidewalls of the nose forming the roof of the nostrils
· The nasal base extends from one side of the nostril to the other along where the nose meets the upper lip.
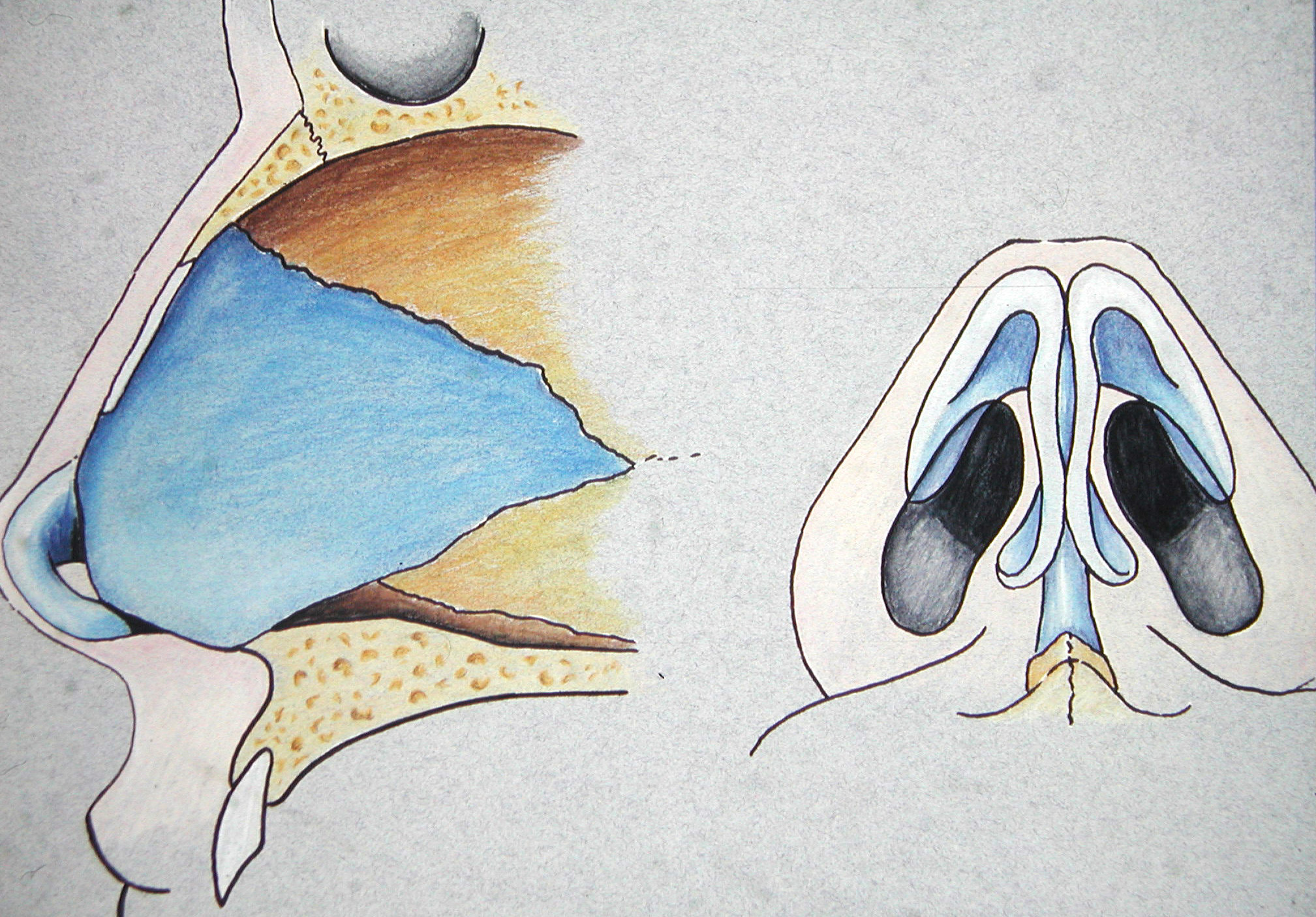
 Beneath this surface topography lies the bone and cartilage structures which give it both shape and support. Some of these important structures are:
Beneath this surface topography lies the bone and cartilage structures which give it both shape and support. Some of these important structures are:
· The paired nasal bones (root and bridge)
· Two upper lateral cartilages (middle vault)
· The septum which runs between the upper lateral cartilages
· Two lower lateral cartilages (tip and nostrils)
· The medial crural footplates (columella)
Contemporary rhinoplasty is focused on conservative and subtle anatomical changes accomplished by preservation, reconstruction and modification of the osseo-cartilaginous framework of the nose. There are two surgical approaches to these structures – the open and the closed approach.
The open approach is performed by making a trans-columellar skin incision combined with internal incisions, followed by skin envelope dissection and elevation. The open approach offers full exposure to the nasal framework, allowing for accurate diagnosis and precise manipulation of its external structures. If extensive changes are needed in a first rhinoplasty or if a secondary rhinoplasty is needed, the open approach is usually better.
The closed approach does not require any skin incision and does not leave external scar since all the incisions are made inside the nose. The lower lateral cartilages can be dissected and freed from the surrounding tissues and “delivered” outside. This approach is best suited for isolated hump deformities or minimal tip changes.
Armed with this basic nose anatomy and surgical terminology, may your rhinoplasty consultation and discussion make you a better educated patient!
Dr. Barry Eppley
Indianapolis, Indiana