

The surgical method for waistline narrowing, behind that of traditional soft tissue removals, is that of rib removal surgery. There are different interpretations of what rib removal surgery is as there is no one definitive technique given the infrequent patient requests and the very few surgeons who actually have any knowledge or actual experience in the procedure.

 In my extensive experience in rib removal surgery for waistline narrowing the operation has evolved to a technique for maximal effectiveness. The removal of the outer half of ribs #10, 11 and 12 is combined with lateral border shaving/excision of the thick latissimus dorsi muscle and flank liposuction. In this approach multilevel tissue reductions are done which optimizes the inward movement of the waistline. It is also a procedure that has been associated with no complications yet seen and less postoperative discomfort and a quicker recovery than one would think. My experience varies greatly from the many myths and misconceptions that have been associated with the surgery.
In my extensive experience in rib removal surgery for waistline narrowing the operation has evolved to a technique for maximal effectiveness. The removal of the outer half of ribs #10, 11 and 12 is combined with lateral border shaving/excision of the thick latissimus dorsi muscle and flank liposuction. In this approach multilevel tissue reductions are done which optimizes the inward movement of the waistline. It is also a procedure that has been associated with no complications yet seen and less postoperative discomfort and a quicker recovery than one would think. My experience varies greatly from the many myths and misconceptions that have been associated with the surgery.
An interesting variation to rib removal (focusing only on the bone manipulation) is whether breaking the ribs (rib fracturing or rib osteotomies) with postoperative molding (corseting) would work. This is an interesting concept that has its theoretical merits…less dissection, shorter operative time and maintenance of rib structure. As a result it bears comparing what is known and not known between the two waistline rib modifications techniques.
Having removed hundreds of ribs for waistline narrowing, and never yet see a single complication or any negative after effects of removing the outer half of ribs #10,11 and 12, I can not speak for whether rib osteotomies vs rib removal is safer or has a quicker recovery.. There simply is no actual clinical information to date by which to compare them. I would imagine that their safety profiles are very similar. For effectiveness the question is not whether rib osteotomies/corseting is better but whether it is just as as effective as rib removals.
 Technically the skin incisions needed to perform either technique would be very similar in location and length. I use a 4.5cm single incision per side to do rib removal surgery which allows access to all three ribs. Whether for removal or fracture this single incision can not be made smaller. I have read that rib fractures can be performed under local anesthesia to which I can say that no form of multiple rib manipulations should be attempted to be performed under local anesthesia. There is no benefit for the patient or the outcome in doing so and may well make the whole experience unpleasant and even less successful for the patient.
Technically the skin incisions needed to perform either technique would be very similar in location and length. I use a 4.5cm single incision per side to do rib removal surgery which allows access to all three ribs. Whether for removal or fracture this single incision can not be made smaller. I have read that rib fractures can be performed under local anesthesia to which I can say that no form of multiple rib manipulations should be attempted to be performed under local anesthesia. There is no benefit for the patient or the outcome in doing so and may well make the whole experience unpleasant and even less successful for the patient.
One of the important elements in rib removal waistline narrowing is the reduction of the thickness of the lateral border of the latissimus dorsi muscle. This soft tissue reduction makes a n unrecognized contribution to waistline narrowing that goes beyond what any change to the rib protrusion/shape does. It is never mentioned in rib fractures whose effects is limited to the bone.
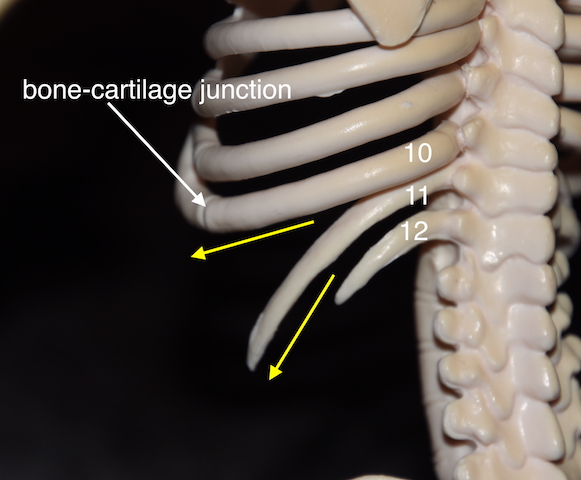
Rib removal has surprisingly less pain afterwards than one would think because there is no bone to heal, it is just a muscle recovery. Whether leaving the ‘fractured’ ribs in place will lead to more postoperative pain or even long-term rib pain as they are trying to heal is a interesting and relevant question. How well do the rib ends heal and do they create some pain while rubbing against each other in so doing. For this reason I would do more than just a fracture line but create a little space between the two ends, ensuring they don’t rub against each other and acknowledging that their healing back together is not functionally important. The rib fracture concept has a theoretical basis for ribs #11 and #12. These are free floating ribs that do not have any end attachments, thus an osteotomy line would allow them to be molded inward. However, this is not a structurally sound concept for rib #10 which is not free floating and attaches around the side to the subcostal rib margin. It would not be able to molded with an osteotomy anywhere along its length. I have learned in rib removal surgery that the most significant waistline effects comes from ribs #10 and #11. Rib #12, the shortest of all ribs in length, has the least impact on the waistline.
The rib fracture concept has a theoretical basis for ribs #11 and #12. These are free floating ribs that do not have any end attachments, thus an osteotomy line would allow them to be molded inward. However, this is not a structurally sound concept for rib #10 which is not free floating and attaches around the side to the subcostal rib margin. It would not be able to molded with an osteotomy anywhere along its length. I have learned in rib removal surgery that the most significant waistline effects comes from ribs #10 and #11. Rib #12, the shortest of all ribs in length, has the least impact on the waistline.
That being said I believe rib osteotomies/fractures have a valid basis for waistline narrowing….which is probably better called ‘rib osteotomy-assisted corseting’. Equally important to the rib cut is the need for great compliance with the corseting. Thus in the properly motivated patient it has a body contouring role. But whether it produces similar results to rib removal surgery is unknown.
Dr. Barry Eppley
Indianapolis, Indiana