


Surgical waistline reduction is most commonly performed by traditional liposuction and tummy tucks. Liposuction has a more profound effect on reducing flank fullness and bringing in the waistline than most tummy tuck in which a horizontal tissue excision is performed with a midline fascial plication. But both together produces the most effective waistline reshaping and is all that most patients need to reach a satisfactory aesthetic result.
More aggressive forms of waistline reshaping exist and fall into the general category of lower lower ribcage modifications. This can be confusing since there are two types of such rib modifications, rib removal and rib fracture. Rib fracture is as the name inplies, a cut is made in ribs #11 and #12. which allows it to be fractured inward. Since the rib is not stabilized inward (plate fixation), it is molded by continuous pressure through a period of months of after surgery corseting. It is the corset that molds the outer half of the rib to curve more inward. Whether it heals by solid osseous healing or fibrous union is not clear. But the fundamental concept is that rib fracture achieves its effect by changing the curve of the lower two ribs only.
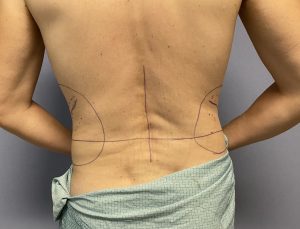
 Rib removal, however, is not quite like the name implies as it is more comprehensive in the waistline tissues that it removes and in the procedures that are involved.. Rib removal involves three types of tissue removals; fat, muscle and bone. The first procedure performed in rib removal is flank liposuction. Even thin people always has some subcutaneous fat that can be removed around the waistline and every little bit of tissue removal helps. Right below the fat lies the very thick and large latissimus dorsi muscle which overlies the lower ribcage. To gain access to the ribs as well as reduce its thickness a large wedge of the outer aspect of the muscle is removed. This has a further waistline narrowing effect.
Rib removal, however, is not quite like the name implies as it is more comprehensive in the waistline tissues that it removes and in the procedures that are involved.. Rib removal involves three types of tissue removals; fat, muscle and bone. The first procedure performed in rib removal is flank liposuction. Even thin people always has some subcutaneous fat that can be removed around the waistline and every little bit of tissue removal helps. Right below the fat lies the very thick and large latissimus dorsi muscle which overlies the lower ribcage. To gain access to the ribs as well as reduce its thickness a large wedge of the outer aspect of the muscle is removed. This has a further waistline narrowing effect.

 The ribs are the last tissues removed and always ribs #11 and #12 have their outer third or more of their length removed. (in some cases rib #10 may also be partially removed if the pleura of the lung is not adherent) This effectively changes the most distal aspect of the rib to a much more proximal location where they no longer push outward on the waistline. The subperiosteal tunnel left behind from the rib removal is packed with a collagen spine soaked in Exparel, a 72 hour acting local anesthetic. This creates some desired numbness of the intercostal nerves, which are dissected out from then rib prior to its removal, as well as that of the surrounding serratus muscles.
The ribs are the last tissues removed and always ribs #11 and #12 have their outer third or more of their length removed. (in some cases rib #10 may also be partially removed if the pleura of the lung is not adherent) This effectively changes the most distal aspect of the rib to a much more proximal location where they no longer push outward on the waistline. The subperiosteal tunnel left behind from the rib removal is packed with a collagen spine soaked in Exparel, a 72 hour acting local anesthetic. This creates some desired numbness of the intercostal nerves, which are dissected out from then rib prior to its removal, as well as that of the surrounding serratus muscles.

 In closing the back incisions for the rib removal procedure a drain may be placed for 24 hours through the liposuction entrance sites in the low back.
In closing the back incisions for the rib removal procedure a drain may be placed for 24 hours through the liposuction entrance sites in the low back.
There are some obvious differences between rib removal and rib fracture which is evident in their names…removing the ribs or bending them in place. One can have a debate about whether they have equal effects on narrowing the waistline which will never be fully answered as a prospective study comparing the two techniques will probably never be done. But the additional tissue removals of fat and muscle give the aesthetic benefit edge to the rib removal approach provided one is prepared for a more invasive surgery and bit longer recovery.
While the two approaches are different it is also possible to merge the two techniques. Through an open approach ribs #10, #11 and #12 can be cut but left them in place as well as remove the latissimus dorsi muscle wedge.
Dr. Barry Eppley
World Renowned Plastic Surgeon