

Background: The surgical origin of a facelift is what transpires around the ears. Making skin incisions around and in (retrotrgal) the ear creates the access needed to both mobilize and reposition loose skin but also to treat the deeper tissue layers. Closing a facelift is about bringing the shape of the ear back out through skin excision and layered tissue suturing.
While much thought and discussion gets into whether and how the SMAS is manipulated in a facelift, incision placement and closure around the ear is often overlooked or taken for granted. One of the underlying principles in removing and redraping facial skin around the ear is to avoid any tension on the lower half of the ear. Since the earlobe contains no supportive cartilage, it is susceptible to being stretched if the skin that is reattached to it is under any tension.
Such elongation of the earlobe after a facelift is known as the pixie ear deformity. While this is a well known term to describe this type of ear deformity, actual pixie ears have elongation of the upper third of the ear and not the lower third. But that issue aside, the vertical lengthening the earlobe and the stretching of the scar around it represents an undesired form of tissue expansion of a once smaller earlobe.
 Case Study: This 62 year-old female had a facelift twelve years previously. As time had progressed she ha lost the benefits of the facelift and was in need of repeat jowl and neck reshaping. One aspect of her original facelift she didn’t like was how it make her ears look. Shortening and reshaping the earlobes was a necessity for her next facelift.
Case Study: This 62 year-old female had a facelift twelve years previously. As time had progressed she ha lost the benefits of the facelift and was in need of repeat jowl and neck reshaping. One aspect of her original facelift she didn’t like was how it make her ears look. Shortening and reshaping the earlobes was a necessity for her next facelift.
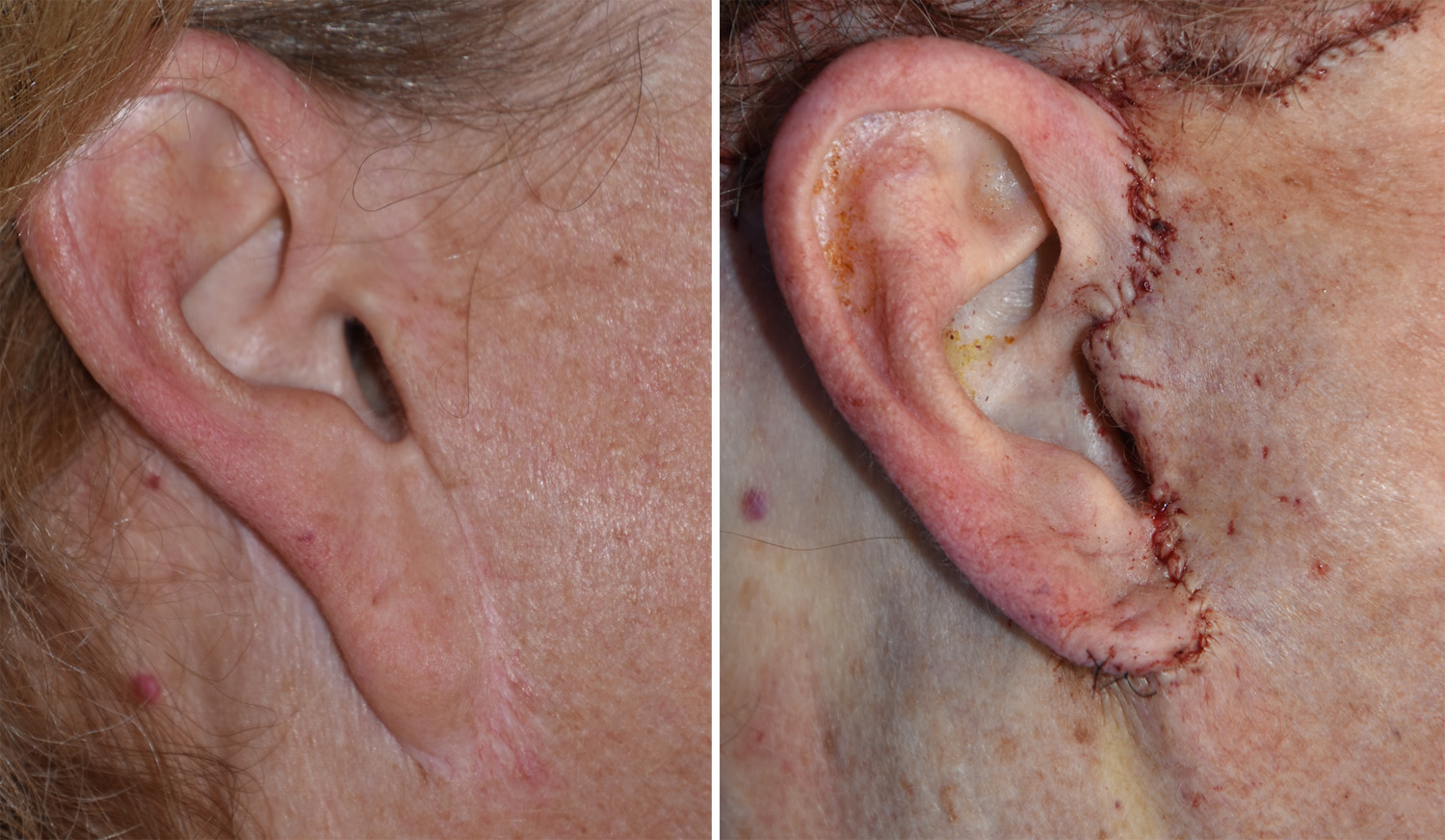
 Under general anesthesia her original facelift and submental incisions were used to perform a secondary facelift with SMAS flap resupension.. As part of the procedure the skin beneath the earlobe was cradled up against the ear cartilage and the earlobes shortened and reattached to it.
Under general anesthesia her original facelift and submental incisions were used to perform a secondary facelift with SMAS flap resupension.. As part of the procedure the skin beneath the earlobe was cradled up against the ear cartilage and the earlobes shortened and reattached to it.
While more minor forms of the pixie ear deformity may be treated by release and vertical skin closure, this will not be effective when the earlobe lengthening is more than 50% of its original length. (unless one can accept a long vertical scar extending down from the earlobe) Wide re-elevation of the facial skin flaps is needed (secondary facelift) for a complete correction with hidden scars.
Highlights:
1) The ear is intimately involved in any facelift procedure.
2) The earlobe contains no cartilage and is susceptible to being elongated after a facelift if any skin tension is placed on it.
3) The severe pixie earlobe deformity is most effectively corrected by a secondary facelift.
Dr. Barry Eppley
Indianapolis, Indiana