

Background: Aesthetic deficiencies of the lower eye/eyelid have a variety of presentations. Dark circles, teat tear troughing, negative vectors and a flat midface describe some of the common terms used to describe the external appearance of a skeletal deficiency of the infraorbital rim or lower eye bone. As a companion to the supraorbital rim or brow bone above it, the infraorbital rim is either at or slightly less forward projecting. When it is less far less horizontally positioned, it is usually associated with other midface hypoplasias of at least the cheek to which it has a common embryologic origin. (zygomatico-orbital complex)
The only standard facial implant that has ever been developed to treat an infraorbital bony deficiency is that of the tear trough implant. Having been around for decades, it is an implant that is designed to fit on the front of the infraorbital rim providing anterior projection and displacing the lower eyelid tissues forward. While effective for the right patient, it is not adequate to treat many other infraorbital deficiencies. It is in fact a one-dimensional trick pony so to speak.
Some lower eyelid bony deficiencies have a vertical component as well. The vertical inter orbital rim distance may be increased as well creating such issues as lack of lower eyelid support, excessive scleral show, fat pseudoherniation and a prominent eye appearance. There are no standard orbital implants that can adequately correct this type of skeletal hypoplasia.
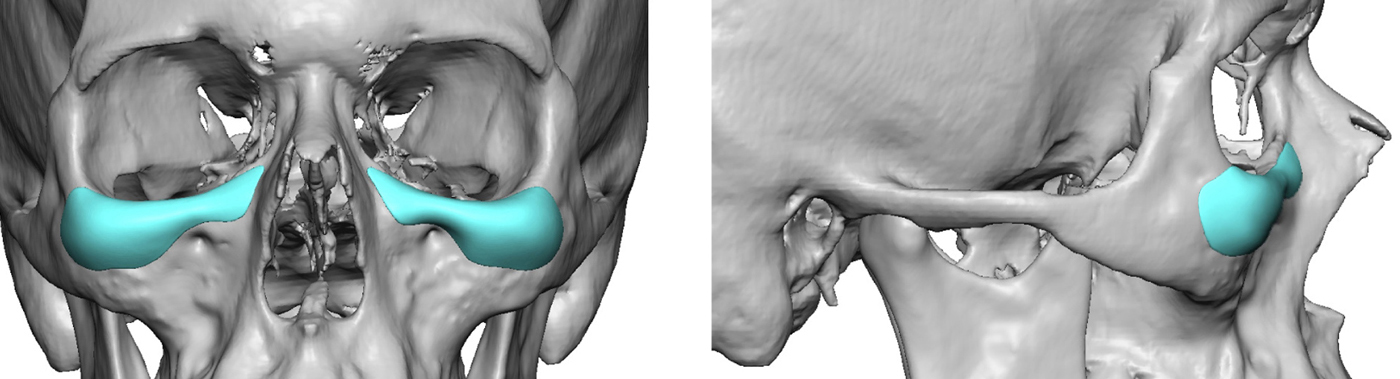 Case Study: This male patient was bothered by his very dark circles and flat area under his eyes. He had a negative vector, flatter cheeks and some false herniation of his lower eyelid fat pads. Custom infraorbital implants were designed to create both horizontal and vertical augmentation of the entire infraorbital rim from side to side. He did not have any concerns about his cheeks so the implant design did not incorporate that skeletal area.
Case Study: This male patient was bothered by his very dark circles and flat area under his eyes. He had a negative vector, flatter cheeks and some false herniation of his lower eyelid fat pads. Custom infraorbital implants were designed to create both horizontal and vertical augmentation of the entire infraorbital rim from side to side. He did not have any concerns about his cheeks so the implant design did not incorporate that skeletal area.

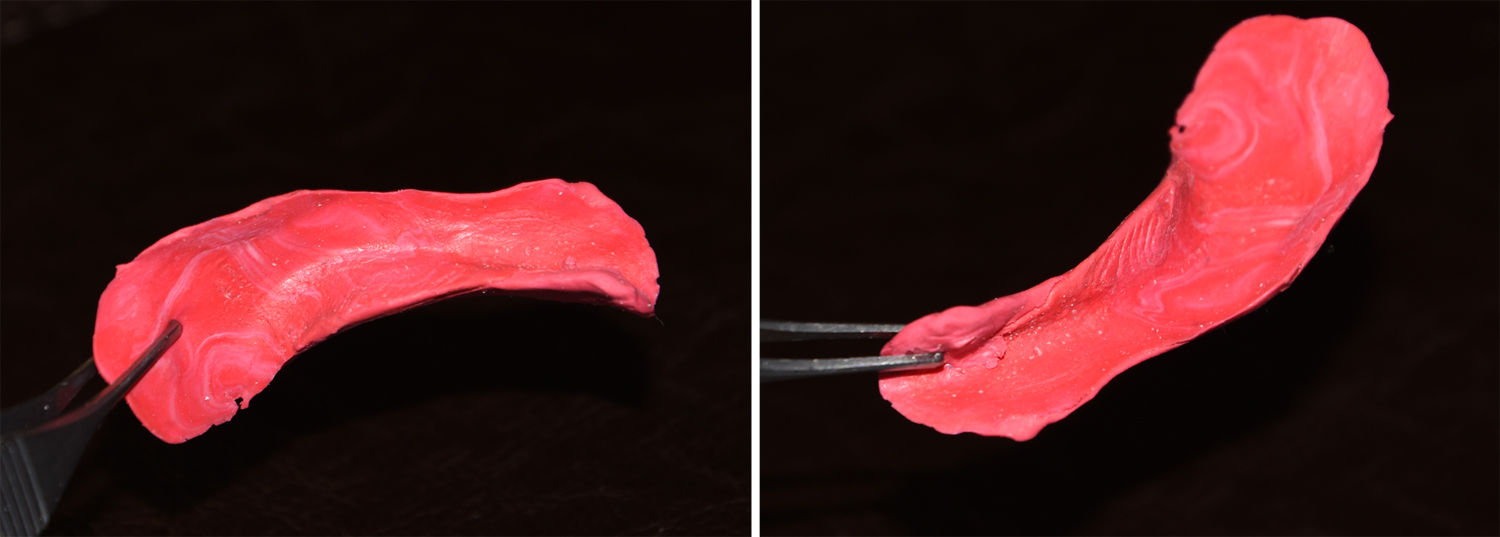 A vertical infraorbital implant has a very unique design feature over that of traditional tear trough implants. The vertical augmentation requires that the implant have a saddle effect across the rim. Thus the implant literally looks like a saddle particularly from the inferior view of it.
A vertical infraorbital implant has a very unique design feature over that of traditional tear trough implants. The vertical augmentation requires that the implant have a saddle effect across the rim. Thus the implant literally looks like a saddle particularly from the inferior view of it.
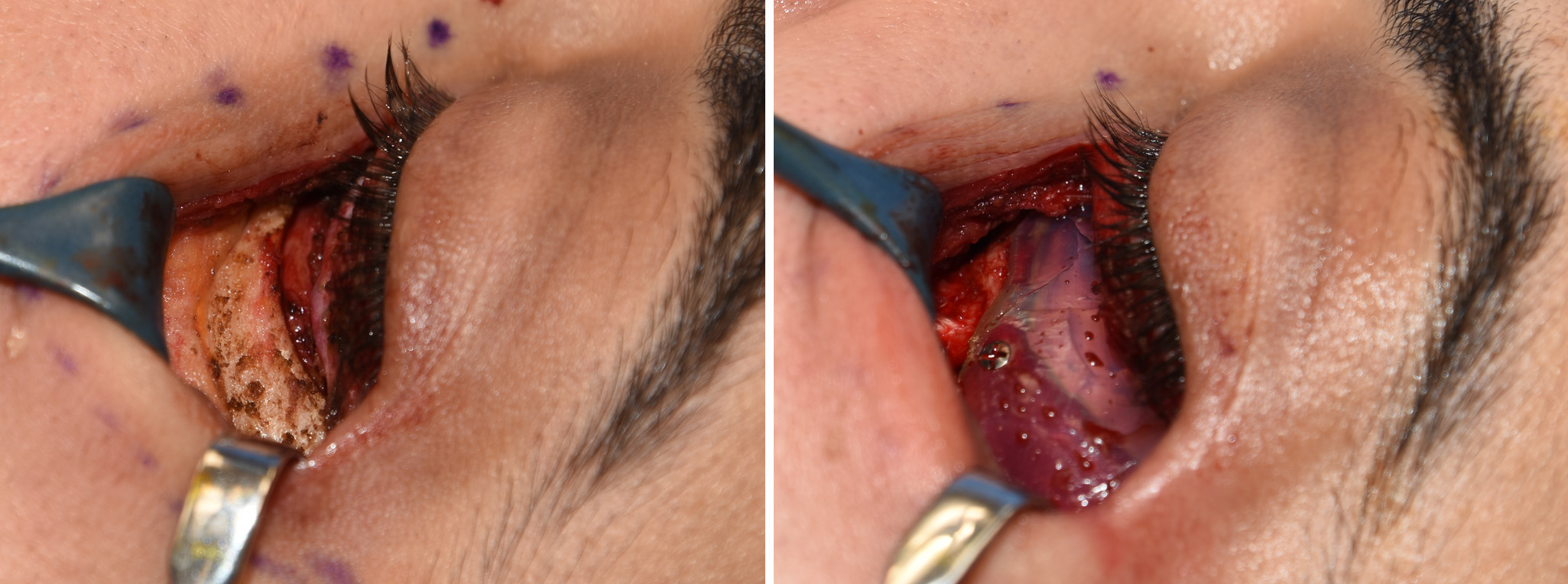 Under general anesthesia a subsidiary lower eyelid incision was made with a small lateral cantonal extension. A skin-muscle flap was raised down to the infraorbital rim with wide subperiosteal undermining with inside and outside of the rim s well as from the nose out to the cheek. The custom infraorbital plants as carved to fit and secured into place with two microscrews per side. Lower eyelid closure consisted of a lateral canthopexy and lateral orbiculares muscle suspension for ectropion prevention.
Under general anesthesia a subsidiary lower eyelid incision was made with a small lateral cantonal extension. A skin-muscle flap was raised down to the infraorbital rim with wide subperiosteal undermining with inside and outside of the rim s well as from the nose out to the cheek. The custom infraorbital plants as carved to fit and secured into place with two microscrews per side. Lower eyelid closure consisted of a lateral canthopexy and lateral orbiculares muscle suspension for ectropion prevention.
The vertical or heightening infraorbital implant requires a custom design and creates a higher level of the natural bony infraorbital rim. In some patients with deep tear troughs, dark circles and infraorbital rim deficiency it is more effective than the traditional tear trough implant.
Highlights:
1) Most orbital rim augmentations provide horizontal projection but not increases in its vertical height of the bone.
2) Some lower eye skeletal deficiencies require increases in the height of the orbital rim wth or without an increase in anterior projection.
3) Only a custom made inferior orbital rim implant can create a decrease in the vertical inter orbital distance.
Dr. Barry Eppley
Indianapolis, Indiana