

Background: Buttock augmentation is most commonly and appropriately done by fat transfer. (BBL) But not every buttock augmentation patient has the needed amount of fat to do a successful procedure nor does fat always survive in a predictable manner. For the thin patient with little fat, buttock implants are the only alternative treatment option. For the failed BBL patient implants also become the alternative approach. I don’t know what percentage of fat injected buttock enhancement patients go on to have implants. But having seen it more than a few times, it clearly is not zero.
While the biggest issue of debate in buttock implants usually revolves around whether their placement should be above (subfascial) or in the muscle (intramuscular) position, this issue actually becomes secondary to implant size. With larger buttock implants sizes, the intramuscular position becomes moot as they simply will not fit into the pocket. And even if they do the muscle over them will atrophy with the pressure and the implant will end up in the subfascial position anyway. While the absolute number on implant size for the intramuscular position differs amongst patients based on their body and buttock size, the range of 400c to 450cc is a good guideline for the upper limit of intramuscular buttock implant size.
If larger buttock implants are desired based on the patient’s goal and the subfascial position is where they will need to be, the issue then becomes the buttock implant itself. Is it if adequate size and shape? While a variety of gluteal implants sizes and shapes exist, some patients may find that their aesthetic needs can not be met by them.
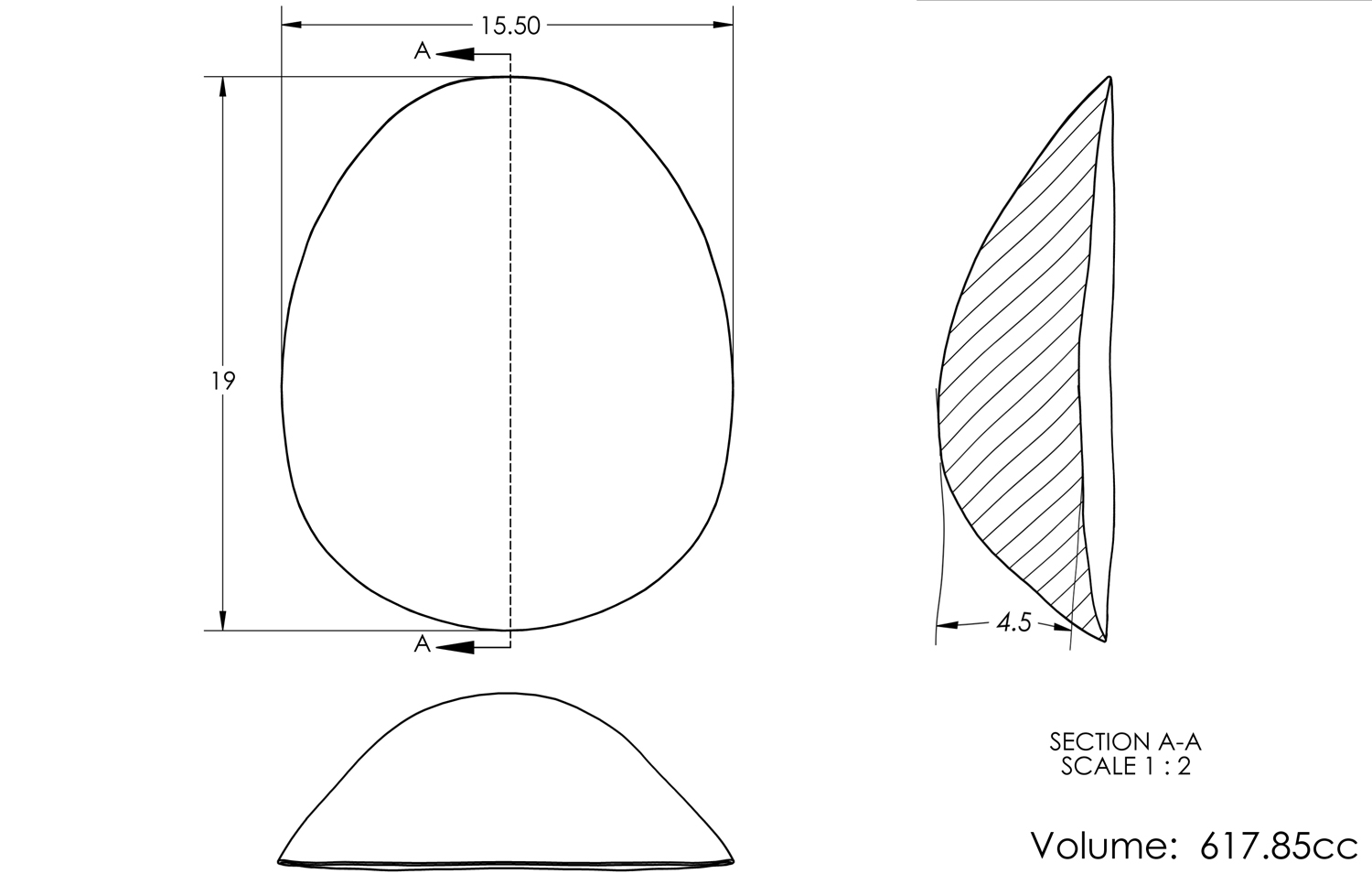 Case Study: This young female had buttock implants placed previously in the subfascial location. While she had no medical problems with them, she did not like their ‘shelving’ effect due to their round profile. Custom implants were designed that were 19 cms in height, 15.5 cms in width and 4.5 cms maximum projection with a total implant volume of almost 620cc. They were anatomic in shape with the maximum projection point being located 1/3 vertical distance from the bottom edge of the implant.
Case Study: This young female had buttock implants placed previously in the subfascial location. While she had no medical problems with them, she did not like their ‘shelving’ effect due to their round profile. Custom implants were designed that were 19 cms in height, 15.5 cms in width and 4.5 cms maximum projection with a total implant volume of almost 620cc. They were anatomic in shape with the maximum projection point being located 1/3 vertical distance from the bottom edge of the implant.
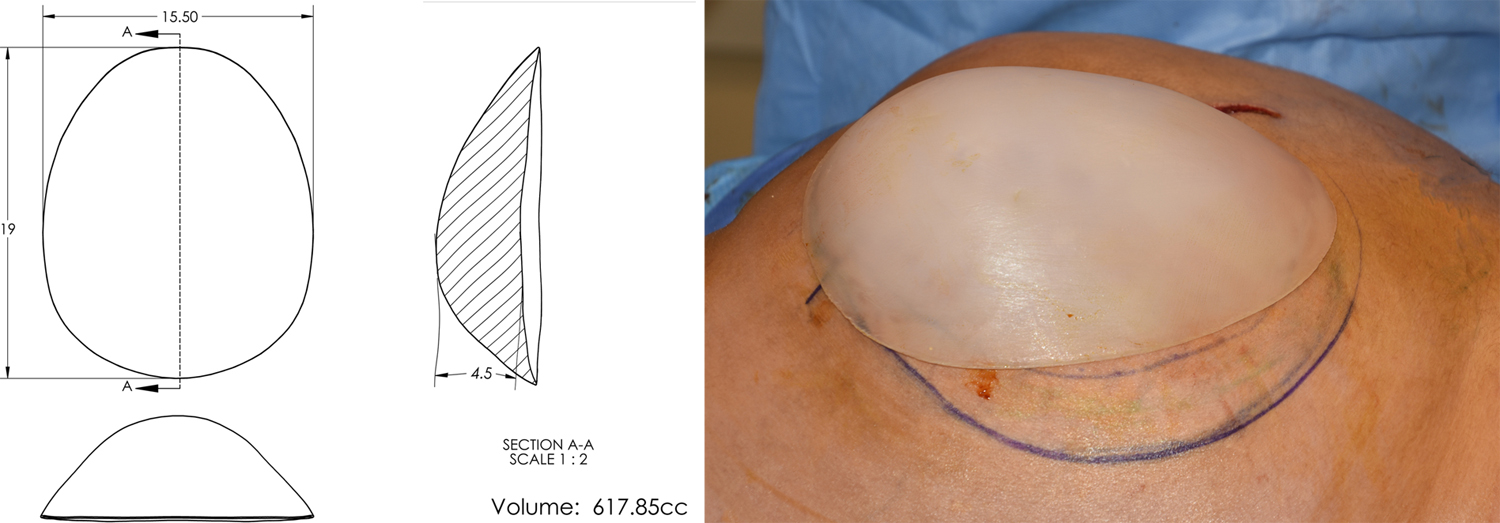
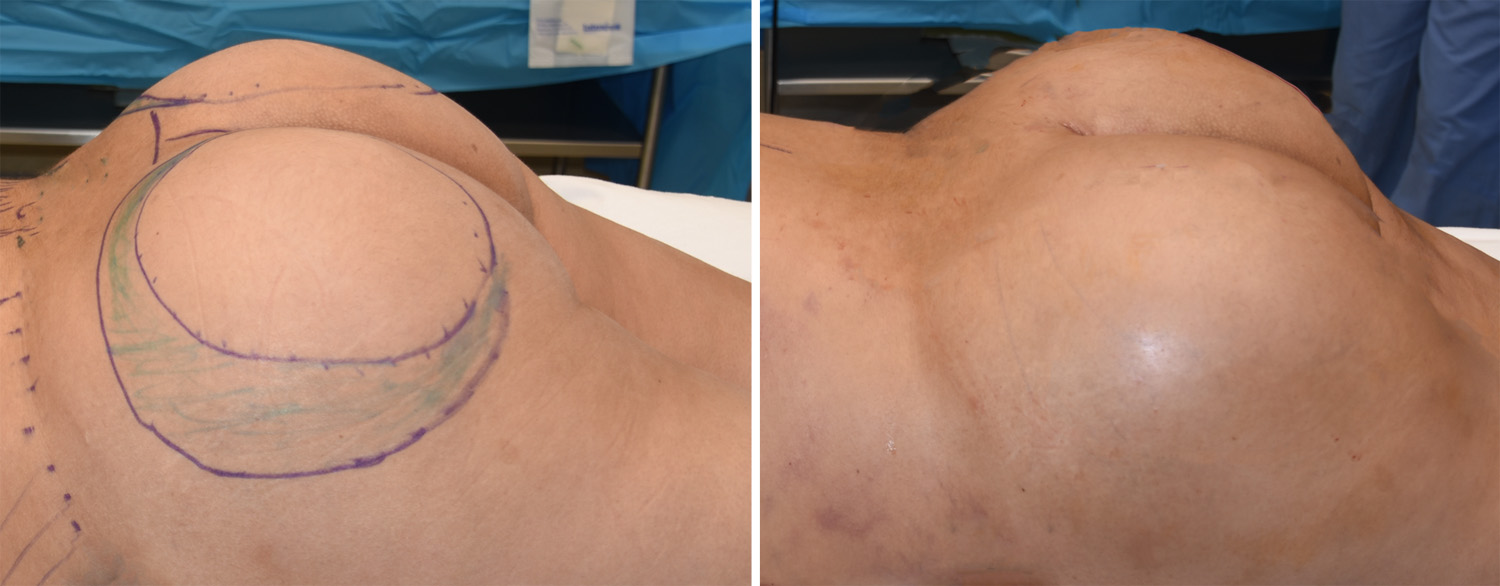 Under general anesthesia the new custom buttock implants replaced her indwelling wound implants with pocket expansion as well. The immediate effects of the implant exchange were obvious with lessening of the round buttock implant look to a more natural shape.
Under general anesthesia the new custom buttock implants replaced her indwelling wound implants with pocket expansion as well. The immediate effects of the implant exchange were obvious with lessening of the round buttock implant look to a more natural shape.
The dimensions of relevance in buttock implants are its size (total volume), shape (round vs anatomic) and the footprint or outline of the implant. Externally what matters is how big does the patient want the buttocks to be, do they want a high round shape or a lower anatomic shape and does the implant go far enough outward towards the hips. When standard buttock implants by their placement has not met the patient’s aesthetic needs, custom replacement implants should able to do so.
Highlights:
1) Custom buttock implants may be needed in some cases of buttock implant replacements to meet the patient’s aesthetic needs.
2) Anatomic buttock implants are useful to decrease a very round buttock shape from prior implants.
3) Custom buttock implants are made in prior implant patients based ink knowing what the indwelling implant dimensions are.
Dr. Barry Eppley
Indianapolis, Indiana