

Background: The buttocks are a frequent site for intramuscular injections due to the large mass and surface area provided by the gluteus maximus muscle. In children it is a particularly preferred injection site. Many different types of injectates can be introduced from antibiotics to vaccinations to steroids. Usually these are few negative side effects from using the buttock injection site.
One known side effect from buttock injections is with the use of steroids. When the dose is too high or placed too superficially the steroid collects in the tissues and creates fat atrophy. This can result in skin dimpling or an indentation. This effect is not seen immediately. It takes several months for it to appear and the progression of its effects may continue for up to six months after the injection.The steroid, triamcinolone (Kenalog), which is widely used is well known to cause this injection site contour deformity.
Reconstruction of buttock injection deformities is one by fat grafting. Whether it would be by injection fat grafting or the use of a composite solid fat graft depends on the size and depth of the indentation.
 Case Study: This 19 year-old female had a left deep buttock scar/indentation from having aa steroid injection done as a child. She had two more superficial ones of the right buttock. The left buttock scar remained deep through her growing years and only became bigger as she got bigger. It was deep and tethered to the underlying muscle.
Case Study: This 19 year-old female had a left deep buttock scar/indentation from having aa steroid injection done as a child. She had two more superficial ones of the right buttock. The left buttock scar remained deep through her growing years and only became bigger as she got bigger. It was deep and tethered to the underlying muscle.
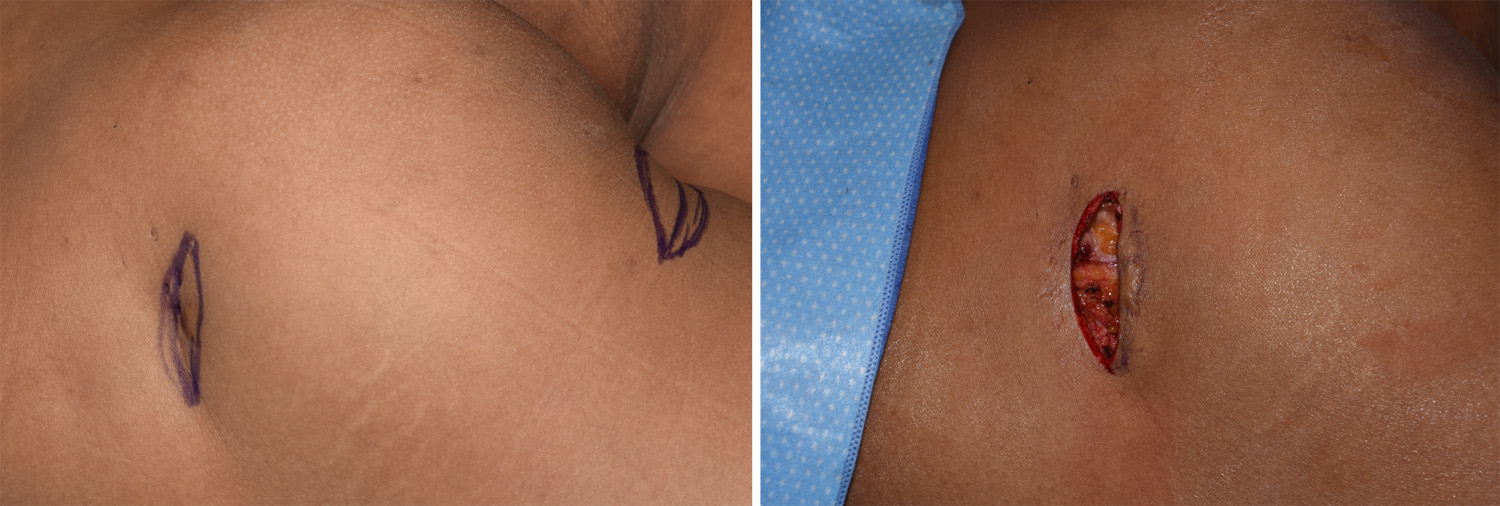

 Under general anesthesia and in the prone position, the buttock scar was excised and the skin widely released. A dermal-fat graft was harvested from the inner infraglutea crease. The overlying epithelium was removed and the grafts was placed dermal side down into the defect. The skin was closed over it. The right buttock scars were treated by fat injections which was harvested from the inner thighs.
Under general anesthesia and in the prone position, the buttock scar was excised and the skin widely released. A dermal-fat graft was harvested from the inner infraglutea crease. The overlying epithelium was removed and the grafts was placed dermal side down into the defect. The skin was closed over it. The right buttock scars were treated by fat injections which was harvested from the inner thighs.
Dermal-fat grafting is an almost forgotten form of soft tissue reconstruction. While injectable fat grafting is far more versatile, there remains a role for composite bloc fat grafting. Scars that are deep and tethered respond better to an open release from which a composite fat graft can be placed. It does require donor site and the infragluteal crease is one option.
Highlights:
1) Buttock indentations are commonly the result of injections.
2) Injectable fat grafting is indicated for less deep and broader-based buttock indentations
3) Buttock indentations that are associated with scar contractors are best treated by release and dermal-fat grafting.
Dr. Barry Eppley
Indianapolis, Indiana