

Deficiences of the infraorbital rim and cheek often appear as under eye hollows. The most common treatments are either synthetic injectable fillers or fat injections for this type of periorbital recession. While effective in many cases, injections may not be permanent or create a uniform appearance. For those patients that seek a permanent solution with more assured smoothness, facial implants can be used. However, there are no performed implants for this area of the periorbital facial skeleton.
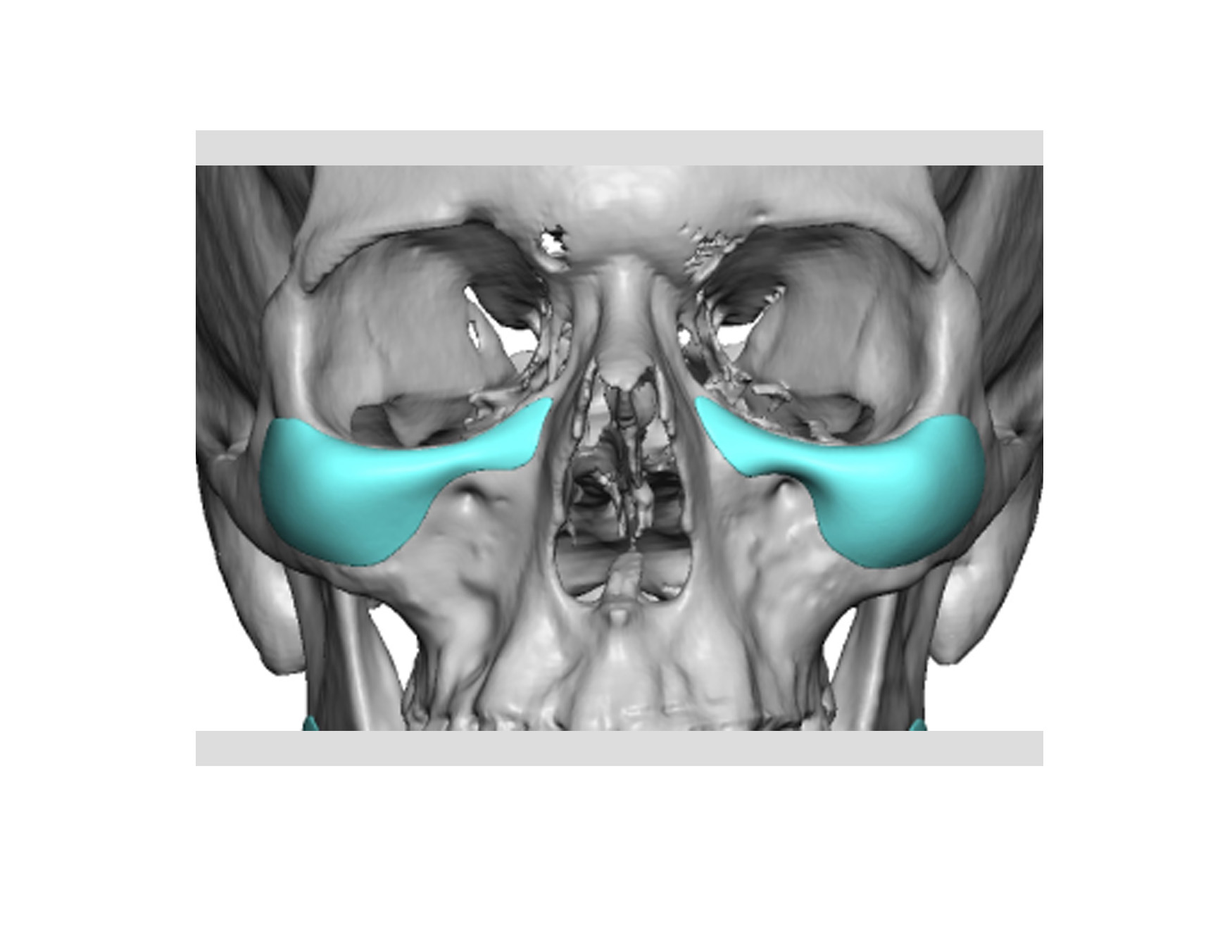 As a result, custom infraorbital malar implants are best choice for the lower eye socket rim and the front part of the cheek. Most infraorbital rim deficiencies, by definition, extend out along the lateral orbital rim on the front part of the zygoma. (cheek) Custom infraorbital malar implants incorporates both adjoining bone areas into its design.
As a result, custom infraorbital malar implants are best choice for the lower eye socket rim and the front part of the cheek. Most infraorbital rim deficiencies, by definition, extend out along the lateral orbital rim on the front part of the zygoma. (cheek) Custom infraorbital malar implants incorporates both adjoining bone areas into its design.
Because of the size of custom infraorbital malar implants, their placement requires an eyelid approach. An intraoral approach is possible but it places the infraorbital nerve at risk for a traction injury and/or malpositioning of the implant. Of the incisional choices between an internal conjunctival or an external subciliary lower eyelid approaches, the external technique is best.
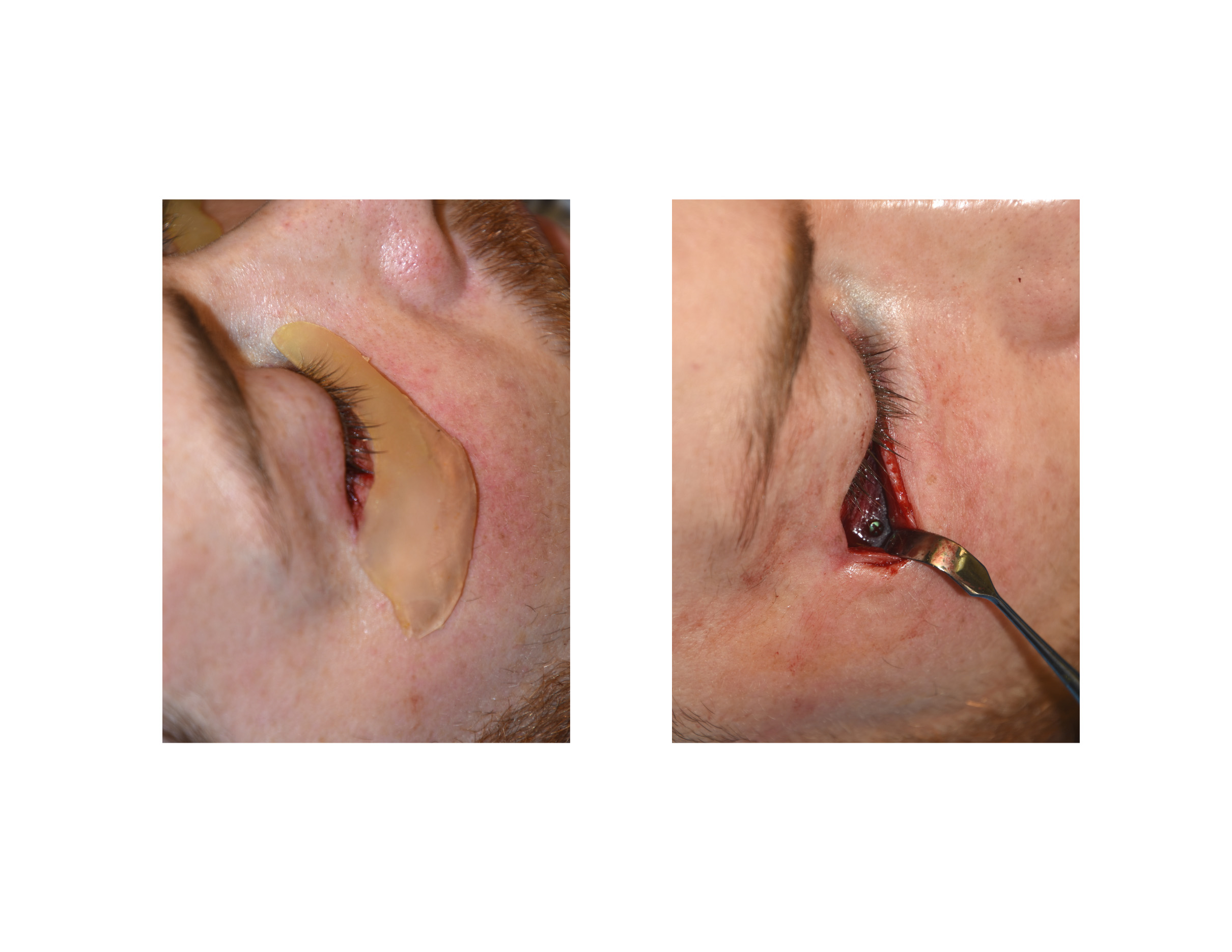
 Through a combined subciilary incision with a small lateral canthal extension, a subperiosteal pocket can be created along the infraorbital rim and zygoma onto the lateral arch. All attached musculature can be elevated and the implant properly positioned. Two small 1.5mm self-drilling screws are used at the medial infraorbital rim and through the junction of the orbital rim and cheek area of the implant. This assures both a tight fit to the bone and assured postoperative implant positioning.
Through a combined subciilary incision with a small lateral canthal extension, a subperiosteal pocket can be created along the infraorbital rim and zygoma onto the lateral arch. All attached musculature can be elevated and the implant properly positioned. Two small 1.5mm self-drilling screws are used at the medial infraorbital rim and through the junction of the orbital rim and cheek area of the implant. This assures both a tight fit to the bone and assured postoperative implant positioning.
Custom infraorbital malar implants provide permanent volume augmentation of the lower periorbital region. A lower eyelid incision with microscrew fixation creates the best positioning for this type of facial implant.
Dr. Barry Eppley
Indianapolis, Indiana