

 Jaw reduction strives to narrow the lower-third of the face, particularly that of the lower jaw and its muscle attachments. There are several techniques for jaw reduction, some surgical and others non-surgical. Jaw reduction is most common in Asians where there is a societal preference for a slender jaw profile. This is in contrast to Causcasians which are more deficient in this area and augmentation is needed rather than reduction.
Jaw reduction strives to narrow the lower-third of the face, particularly that of the lower jaw and its muscle attachments. There are several techniques for jaw reduction, some surgical and others non-surgical. Jaw reduction is most common in Asians where there is a societal preference for a slender jaw profile. This is in contrast to Causcasians which are more deficient in this area and augmentation is needed rather than reduction.
 One form of jaw reduction involves surgical reduction of the mandible or lower jaw angle area. Done through an incision inside the mouth, the jaw angle (junction of the back part of the jaw and the lower border of the jaw) is essentially sawed off. This changes the sharp acute angle of the jaw to a more round one. This softens the jaw angle and raises the line of the jaw from front to back. The bone cut can be extended from the jaw angle forward to about the middle of the body of the jaw for greater narrowing. Another bony reduction option is an outer corticotomy. Rather than just saw off the entire jaw angle, which can really blunt the angles and cause loss of soft tissue support, is to remove just the outer cortex of the angle area. Done lije a reverse sagittal split osteotomy, this will thin out the jaw angle are but without blunting the angle.
One form of jaw reduction involves surgical reduction of the mandible or lower jaw angle area. Done through an incision inside the mouth, the jaw angle (junction of the back part of the jaw and the lower border of the jaw) is essentially sawed off. This changes the sharp acute angle of the jaw to a more round one. This softens the jaw angle and raises the line of the jaw from front to back. The bone cut can be extended from the jaw angle forward to about the middle of the body of the jaw for greater narrowing. Another bony reduction option is an outer corticotomy. Rather than just saw off the entire jaw angle, which can really blunt the angles and cause loss of soft tissue support, is to remove just the outer cortex of the angle area. Done lije a reverse sagittal split osteotomy, this will thin out the jaw angle are but without blunting the angle.
One thing that bony jaw angle reduction of any method does not do is correct for the thickness of the muscle over the bone. It is not really possible (or desireable if you are the patient) to surgically thin out the muscle without causing a lot of pain and causing long-term restriction of mouth opening. Therefore, the effectiveness of jaw angle reduction will be more or less dependent on the how much the bone of the jaw causes the fullness of the jaw angle. That being said, bony jaw angle reduction will always make a visible external difference.
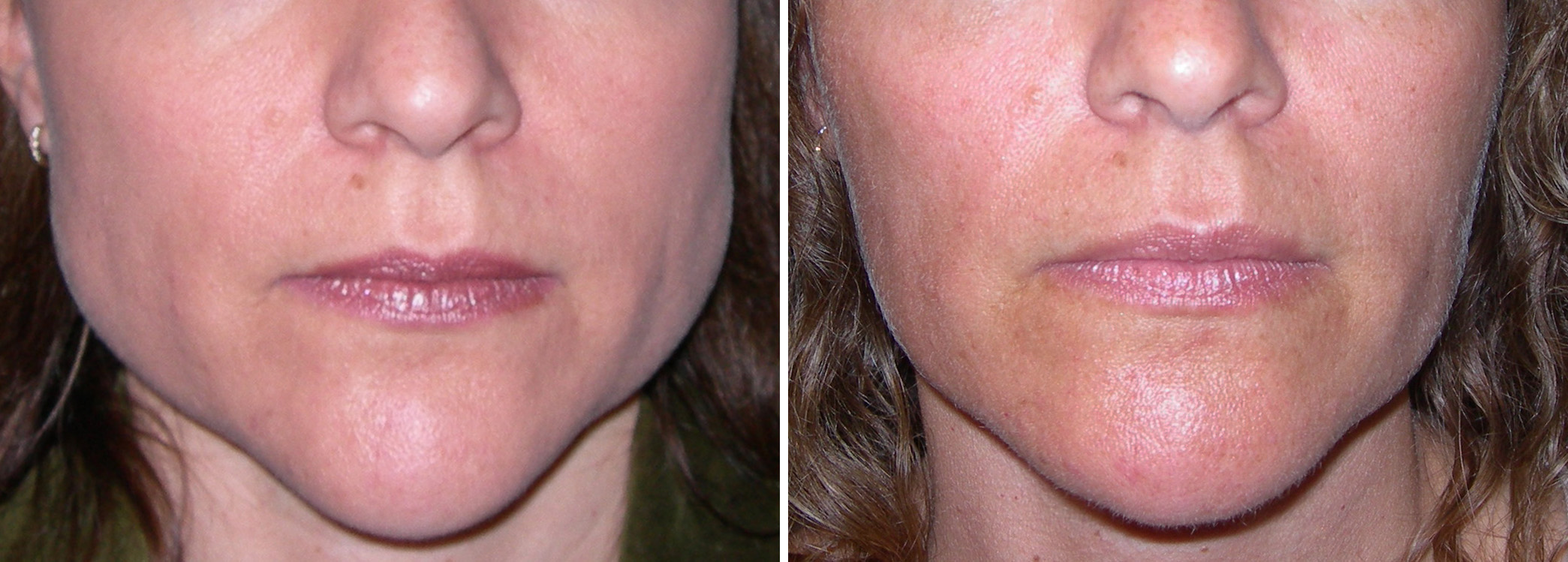 Non-surgical jaw angle reduction means Botox® injections. While this muscle paralyzing drug initially seems like it would not work for long-term muscle reduction (atrophy), it has been shown that it actually does. The dose of Botox® is fairly high for each side ( about 40 to 50 units), and it must be repeated every 4 months or so for up to a year or longer, but I have witnessed the masseter muscle actually get smaller over time. Why the muscle shrinks when it is partially paralyzed (chewing function is not affected) is not known and the next question is….will it stay smaller long after the Botox® injections are stopped. Proponents of this injection technique say that it does but long-term clinical studies have never been reported as of yet.
Non-surgical jaw angle reduction means Botox® injections. While this muscle paralyzing drug initially seems like it would not work for long-term muscle reduction (atrophy), it has been shown that it actually does. The dose of Botox® is fairly high for each side ( about 40 to 50 units), and it must be repeated every 4 months or so for up to a year or longer, but I have witnessed the masseter muscle actually get smaller over time. Why the muscle shrinks when it is partially paralyzed (chewing function is not affected) is not known and the next question is….will it stay smaller long after the Botox® injections are stopped. Proponents of this injection technique say that it does but long-term clinical studies have never been reported as of yet.
Dr. Barry Eppley
Indianapolis, Indiana