

Pectoral implants, although far less commonly done than breast implants, share some similarities with its more well known female counterpart. The implant pocket location is almost the same (submuscular) and the location of the incision is one that is often used in breast implants as well. (transaxillary)
 But beyond these two similarities the male and female chest enhancement procedures differ. They most noteworthy difference is in the implants themselves. Unlike breast implants which are round and are fluid or gel filled, pectoral implants are more rectangular in form and are made of a solid but ultrasoft silicone material. As a result pectoral implants will never break down or need to be replaced due to device failure. (rupture)
But beyond these two similarities the male and female chest enhancement procedures differ. They most noteworthy difference is in the implants themselves. Unlike breast implants which are round and are fluid or gel filled, pectoral implants are more rectangular in form and are made of a solid but ultrasoft silicone material. As a result pectoral implants will never break down or need to be replaced due to device failure. (rupture)
A less noticeable but tremendously important difference is the differences in the submuscular pocket. Breast implants, in an effort to get a round or teardrop shape, almost always have the outer side of the implant going beyond the lateral border of the pectoral muscle. (known as a dual plane placement….partial submuscular and partial subcutaneous pocket) This not only makes for a rounder shape but also strives to keep the nipple in the center of the enlarged breast mound. Conversely such a pocket location will not work for pectoral implants because it needs a shape that closely matches the shape of the pectoral muscle which is more rectangular. And in which the nipple is located at the bottom of the augmented chest at the inferolateral pectoral muscle border.
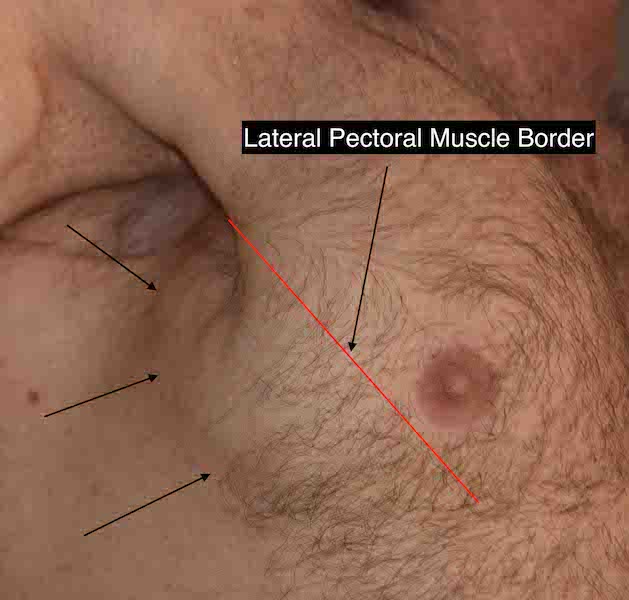
 The single most common pectoral implant problem that I see from other surgeons is that the implant violates the lateral pectoral border. This creates an obvious implant bulge that sticks out below and beyond the muscle which is obvious unnatural. Such lateralization of the pectoral implant can result in loss of volume along the medial sternal border. This can occur from either over dissection of the lateral muscle border during placement or having implant dimensions which do not match the width of they pectoral muscle.
The single most common pectoral implant problem that I see from other surgeons is that the implant violates the lateral pectoral border. This creates an obvious implant bulge that sticks out below and beyond the muscle which is obvious unnatural. Such lateralization of the pectoral implant can result in loss of volume along the medial sternal border. This can occur from either over dissection of the lateral muscle border during placement or having implant dimensions which do not match the width of they pectoral muscle.
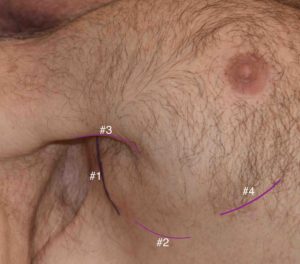 The decisions to make in treating lateral pectoral implant displacement is 1) where to place the incision, 2) should the medial pocket be opened further and the implant repositioned with lateral capsular plication or 3) reduce the protruding lateral part of the implant with lateral capsular plication. For the incision there are four different options of which none is necessarily better than the other. There are just different locations none of which is true completely hidden. What is known for sure is that it is very difficult if not possible to use the original transaxillary incision for any manipulation of the implant or its pocket.
The decisions to make in treating lateral pectoral implant displacement is 1) where to place the incision, 2) should the medial pocket be opened further and the implant repositioned with lateral capsular plication or 3) reduce the protruding lateral part of the implant with lateral capsular plication. For the incision there are four different options of which none is necessarily better than the other. There are just different locations none of which is true completely hidden. What is known for sure is that it is very difficult if not possible to use the original transaxillary incision for any manipulation of the implant or its pocket.
Both pocket adjustment/implant repositioning and implant trimming can be successful, both of which employ lateral capsular plication. This decision is most driven by the symmetry of the shape of the chest augmentation near the sternum. If the two sides are fairly similar, removing the implant protrusions would be the most successful. If the medial chest wall is asymmetric/lacks volume then pocket release and medializing the implant is needed.
Dr. Barry Eppley
Indianapolis, Indiana