

Aesthetic skull augmentation refers to adding a material on top of the outer cranial surface (onlay) to create a change in the shape of the head. This concept can be applied any of the five skull surfaces. (front, back, sides and top) This should not be confused with the more well known techniques used in skull reconstruction from traumatic injuries and craniotomies. In these skull applications reconstruction or replacement of portions of the bone is done in which some similar materials but different techniques are used.

 Bone cements have historically been used for aesthetic onlay skull augmentations because they already existed and surgeons were familiar with them. Whether this was either PMMA (acrylic) or HA (hydroxyapatite), these liquid and powder formulations create a putty which can be applied, shaped and allowed to harden. Such bone cements were developed and FDA-approved for placement into skull bone defects. There are used in aesthetic skull augmentation as an off-label indication and are much more technique sensitive to develop their shapes than when placed into self-contained bone defect in which they were actually developed to do so.
Bone cements have historically been used for aesthetic onlay skull augmentations because they already existed and surgeons were familiar with them. Whether this was either PMMA (acrylic) or HA (hydroxyapatite), these liquid and powder formulations create a putty which can be applied, shaped and allowed to harden. Such bone cements were developed and FDA-approved for placement into skull bone defects. There are used in aesthetic skull augmentation as an off-label indication and are much more technique sensitive to develop their shapes than when placed into self-contained bone defect in which they were actually developed to do so.

 The use of various implant materials (HTR, PEEK, PEKK) in the skull have only FDA-approved uses for inlay or skull defect reconstructions. Because of their preformed shapes they are made from 3D CT scans of the skull defect. While any of these implant materials can be used for aesthetic skull augmentation they pose significant cost and application challenges. As a result solid silicone is a far more friendly skull augmentation material in which the challenges of cost and application are overcome. Solid silicone also has the longest history of use in both aesthetic face and body augmentations. A custom approach is still needed using the patient’s 3D CT scan and their use in this regard falls under the FDA approval guidelines of a custom implant device that is individually made for each patient.
The use of various implant materials (HTR, PEEK, PEKK) in the skull have only FDA-approved uses for inlay or skull defect reconstructions. Because of their preformed shapes they are made from 3D CT scans of the skull defect. While any of these implant materials can be used for aesthetic skull augmentation they pose significant cost and application challenges. As a result solid silicone is a far more friendly skull augmentation material in which the challenges of cost and application are overcome. Solid silicone also has the longest history of use in both aesthetic face and body augmentations. A custom approach is still needed using the patient’s 3D CT scan and their use in this regard falls under the FDA approval guidelines of a custom implant device that is individually made for each patient.
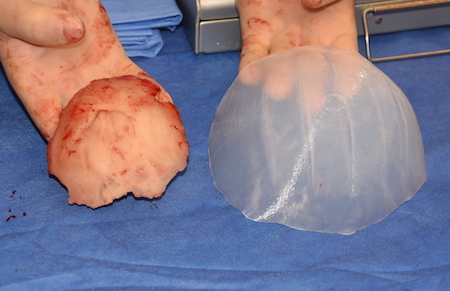
While both bone cements and custom silicone implants can be used for skull augmentation, their aesthetic effects and placement techniques differ significantly. Both materials types have similar biocompatibility and infection risks but they differ in shape control, surface area coverage, scalp incision length, risk of revision for aesthetic reasons, ease of secondary modification/replacement and cost.
This is best understood by the following comparison table on a 1 to 4 rating scale. (4+ = best, 1+ = worst)
Property Bone Cements Custom Implants
Shape Control ++ ++++
Surface Area Coverage + ++++
Scalp Incision Length +. ++++
Aesthetic Revision Risk ++ ++++
Ease of
Modification/Replacement. + ++++
Cost +++ ++
TOTAL 10 22
 To best summarize these differences bone cements require much larger scalp incisions for placement, have less skull surface area coverage with reduced assurance of shape control and achieving the desired augmentation effect.As a result, bone cements have a much higher rate of revision and are more difficult to modify or replace. Conversely custom skull implants initially cost more but offer greater assurance of the desired aesthetic result due to the preoperative design process. As a result a much lower revision rate exists which justifies the increased implant cost.
To best summarize these differences bone cements require much larger scalp incisions for placement, have less skull surface area coverage with reduced assurance of shape control and achieving the desired augmentation effect.As a result, bone cements have a much higher rate of revision and are more difficult to modify or replace. Conversely custom skull implants initially cost more but offer greater assurance of the desired aesthetic result due to the preoperative design process. As a result a much lower revision rate exists which justifies the increased implant cost.
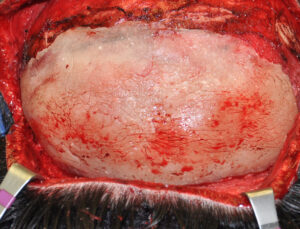
The major problem with bone cements is the need to have a much larger incision to place them. This is a significant impediment to their use. Incisions can be made much smaller like those used in custom skull implants but then control is lost of implant shape. The other issue with limited scalp incisions with bone cements is that the recoil of the scalp pushes back one the cement and only limited amounts of skull augmentation can be obtained. Conversely the preformed shape and thickness of a custom implant pushes back on the scalp recoil/tightness and pushes out much more effectively.
Dr. Barry Eppley
Indianapolis, Indiana