


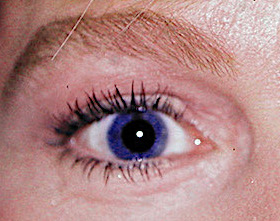
 The lower eyelid is composed of three tissue layers known as the lamella. There is an outer layer (skin), middle layer (muscle and fascia) and inner lamellar layer. (mucosa) Changes occur from youth to older age in all eyelid layers of which the most noticeable is the skin. In youth the lower eyelid skin is taut with few wrinkles and often has a roll of tissue right under the lashes. This linear puffiness under the lashes is due to the thickness of the orbicularis muscle. Some people’s are thicker than others so the size of this roll is very variable
The lower eyelid is composed of three tissue layers known as the lamella. There is an outer layer (skin), middle layer (muscle and fascia) and inner lamellar layer. (mucosa) Changes occur from youth to older age in all eyelid layers of which the most noticeable is the skin. In youth the lower eyelid skin is taut with few wrinkles and often has a roll of tissue right under the lashes. This linear puffiness under the lashes is due to the thickness of the orbicularis muscle. Some people’s are thicker than others so the size of this roll is very variable
 When younger this muscle roll is larger and makes the skin taut with less wrinkles. But as we age the orbicularis muscle thins and the skin sags making this area under the eye look sunken. In certain cultures (e.g., Asian) having a more prominent under eyelid roll is associated with youthfulness and beauty. Its prominence in Western cultures is less valued as aesthetically significant.This lower eyelid area can be augmented and is known as love band surgery. It is intended to mimic the youthfulness that naturally occurs in the skin just below the eyelashes.It is also known as Aegyo Sal in Asia which when translated means ae (love), gyo (beautiful) and sal. (skin)
When younger this muscle roll is larger and makes the skin taut with less wrinkles. But as we age the orbicularis muscle thins and the skin sags making this area under the eye look sunken. In certain cultures (e.g., Asian) having a more prominent under eyelid roll is associated with youthfulness and beauty. Its prominence in Western cultures is less valued as aesthetically significant.This lower eyelid area can be augmented and is known as love band surgery. It is intended to mimic the youthfulness that naturally occurs in the skin just below the eyelashes.It is also known as Aegyo Sal in Asia which when translated means ae (love), gyo (beautiful) and sal. (skin)
 This augmentation can be done with injections using synthetic fillers and fat, Alloderm (tissue back dermis) grafts or implants. (ePTFE) While injections can produce an immediate result, they are non-lasting. Alloderm grafts are the most widely used even though it is a surgical procedure because of its longer lasting effects and suppleness of the graft material. I prefer the thickness of the Alloderm to be in the 2mm range, anything less will not be very visible.
This augmentation can be done with injections using synthetic fillers and fat, Alloderm (tissue back dermis) grafts or implants. (ePTFE) While injections can produce an immediate result, they are non-lasting. Alloderm grafts are the most widely used even though it is a surgical procedure because of its longer lasting effects and suppleness of the graft material. I prefer the thickness of the Alloderm to be in the 2mm range, anything less will not be very visible.
 The love band procedure can be done under local anesthesia or IV sedation by itself but is more commonly combined with other procedures under general anesthesia. The technique is done by making two small incisions at both ends of the desired roll effect. A 5mm skin incision is made in the lateral canthal skin crease and a 3mm horizontal incision at the medial or inner side of the desired roll. A subcutaneous tunnel is made between the two incisions with small scissors or elevator.
The love band procedure can be done under local anesthesia or IV sedation by itself but is more commonly combined with other procedures under general anesthesia. The technique is done by making two small incisions at both ends of the desired roll effect. A 5mm skin incision is made in the lateral canthal skin crease and a 3mm horizontal incision at the medial or inner side of the desired roll. A subcutaneous tunnel is made between the two incisions with small scissors or elevator.
 The Alloderm graft has the general dimensions of 3.5mms in height centrally with tapered ends. It is usually advised to taper the bottom edge with scissors once fully hydrated. Make the graft longer than initially desired and trim the ends after placement.
The Alloderm graft has the general dimensions of 3.5mms in height centrally with tapered ends. It is usually advised to taper the bottom edge with scissors once fully hydrated. Make the graft longer than initially desired and trim the ends after placement.
 The graft can be passed through by multiply methods by using a suture technique to pull it through is the easiest in my experience. The protruding ends can then be trimmed prior to closure, making sure the very end of the graft is well buried under the skin closure. Rapidly dissolving 6-0 plain sutures are used with the medial ends trimmed very short to avoid corneal contact.
The graft can be passed through by multiply methods by using a suture technique to pull it through is the easiest in my experience. The protruding ends can then be trimmed prior to closure, making sure the very end of the graft is well buried under the skin closure. Rapidly dissolving 6-0 plain sutures are used with the medial ends trimmed very short to avoid corneal contact.
There is always the question of the persistence of Alloderm grafts which do have a poor track record in the lips. But my experience in the eyelids has been different perhaps because it is a less dynamic structure and the graft-recipient site size ratio is much larger.
Dr. Barry Eppley
Indianapolis, Indiana