

Background: The face is prone to fat loss that classically affects the temporal and cheek areas. The fat that lies within the temporal muscle above the zygomatic arch and the fat compartments below the cheekbones can undergo volume loss due to a variety of medical conditions/drugs, aging, weight loss and surgery. Such effects are more prone to occur in naturally thinner or more lean faces.
The most recognized facial area where this occurs is in the temporal areas by the side of the eye. This area is particularly prone to fat due to the contribution of an extension of the buccal fat pad. Such temporal hollowing can be treated by injectable fillers, fat injections or standard temporal implants. When fat harvest sites have been depleted or has not worked well, temporal implants provide an effective surgical solution that provides assured volume retention. The use of extended temporal implant designs works will for most females as the hollowing extends all the way to the top of the bony temporal line.
Fat loss in the face below the zygomatic arches typically affects the cheek fat of the buccal fat pad and the subcutaneous fat in the more anterior cheek areas with a resultant concave contour. But there is another source for a facial concave effect….a facelift. The pullback of the lateral facial skin and SMAS towards the ear can create a sweepback look to the face in thinner patients. This is a well known aesthetic effect of the procedure that can occur in some patients. While some may not mind it or even find to be a beneficial effect, some females may not as the hollowing effect may make one look a bit older. How to treat this aesthetic issue when fat is not available has not been previously reported.
 Case Study: This female was bothered by the reverse hourglass shape of her face with temporal hollowing above the zygomatic arches and a concavity on the sides of her face immediately below it. The surgical goal was to augmented the temporal and facial hollowing with implants since she had prior liposuction for various effects and her fat harvest sites were very limited. In addition she preferred an implant augmentation method because of its assured and persistent augmentation effect.
Case Study: This female was bothered by the reverse hourglass shape of her face with temporal hollowing above the zygomatic arches and a concavity on the sides of her face immediately below it. The surgical goal was to augmented the temporal and facial hollowing with implants since she had prior liposuction for various effects and her fat harvest sites were very limited. In addition she preferred an implant augmentation method because of its assured and persistent augmentation effect.

 Under general anesthesia the extended temporal implants were placed through a high small incision inside the temporal hairline in the subfascial location. Some reduction of its length was necessary due to her distance between the bony temporal line and the zygomatic arch.
Under general anesthesia the extended temporal implants were placed through a high small incision inside the temporal hairline in the subfascial location. Some reduction of its length was necessary due to her distance between the bony temporal line and the zygomatic arch.



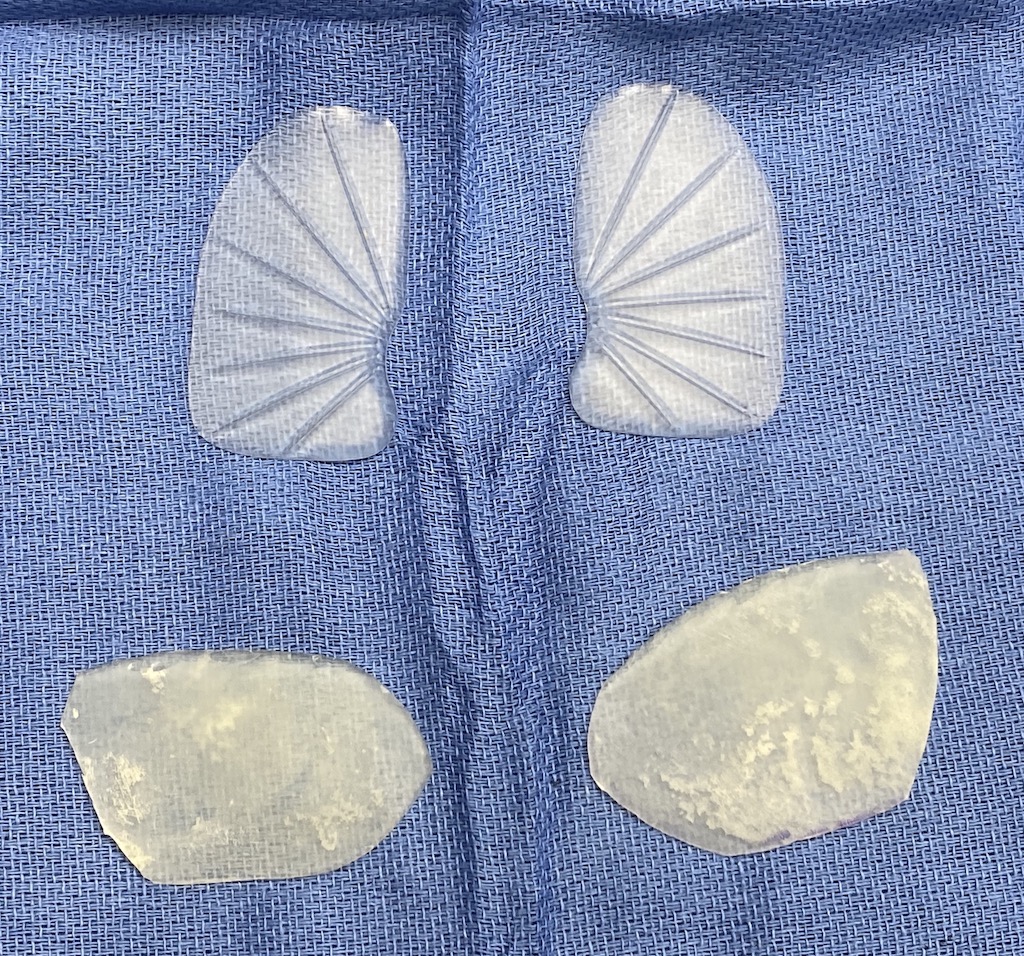
 Then through her prior preauricular (and retrotragal) incisions a skin flap was developed over and around the facial concavity in front of the ear. The facial implants were hand fashioned from 2mm thickness soft solid silicone sheeting whose shape was based on paper templates taken from the facial markings. Multiple 2mm perfusion holes were placed through the implants to allow for tissue ingrowth. The implants were placed under the skin flap and sutured into place.
Then through her prior preauricular (and retrotragal) incisions a skin flap was developed over and around the facial concavity in front of the ear. The facial implants were hand fashioned from 2mm thickness soft solid silicone sheeting whose shape was based on paper templates taken from the facial markings. Multiple 2mm perfusion holes were placed through the implants to allow for tissue ingrowth. The implants were placed under the skin flap and sutured into place.
 The volumetric effect was smooth and modest (2 to 3mms in thickness) which was all that a thin face needs in these non-bony soft tissue supported facial areas.
The volumetric effect was smooth and modest (2 to 3mms in thickness) which was all that a thin face needs in these non-bony soft tissue supported facial areas.
The use of temporal implants for their hollowing corrective benefits is well known. Placing an implant in the subcutaneous tissues of the face is not. But that doesn’t mean it can not be effective for filling smaller areas of volume loss. Such implants are an option when fat grafting is not possible or desired.
Case Highlights:
1) Temporal hollowing occurs from fat loss caused by aging, natural genetics or medical conditions that result in facial lipoatrophy.
2) Facelift surgery, particularly if done multiple times, can have a thinning effect on the side of the face beneath the cheekbone back to the ear.
3) If fat grafting is not an option or has failed implants can be used for the temporal and facial contour concavities.
Dr. Barry Eppley
Indianapolis, Indiana