

Background: The skull can develop various areas of flatness or underdevelopment. Such flat areas of the head are particularly common on the back of the head. While the most common back of the head deficiency is due to plagiocephaly, with one side of the back of the head being flat, such lack of skull projection can also occur bilaterally. (Brachycephaly) Such brachycephalic skull shapes are not uncommon in Asian ethnicities where the back of the head can be flat and excessively wide as well.
In adults the aesthetic treatment of brachycephaly is onlay skull augmentation. The most effective method to treat such skull shape deficiencies is a custom skull implant designed from the patient’s 3D CT scan. In designing such skull implants the question is always how much projection can be added to the back of the head. This is a function of how much the scalp can stretch to accommodate the implant volume beneath it. My experience is that up to 150ccs of implant volume can be accommodated in deficient skull areas. This limitation is based on the use of a small incision for access which does not allow the same scalp stretch that could be developed with a trans coronal scalp incision. But the scar burden of such a long scalp incision is not a good aesthetic tradeoff to be able to fit a bigger skull implant.
While brachycephaly most commonly affects the back of the head it also can affect the forehead as well. The forehead can also lack forward projection although the amount of forward growth deficiency is often less than that on the back of the head. Custom skull implants can be made for both the front and back of the skull and can be placed concurrently.
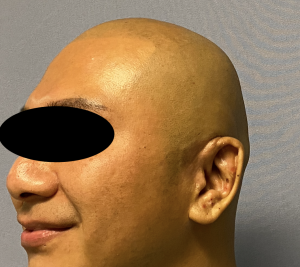
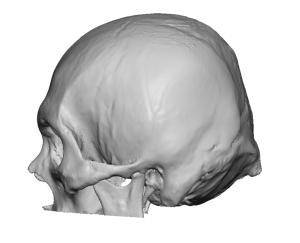 Case Study: This male was bothered primarily by the flatness on the back of the head and secondarily on his forehead. The back of his head appeared to be cut off and his 3D CT scan confirmed the degree of flatness.
Case Study: This male was bothered primarily by the flatness on the back of the head and secondarily on his forehead. The back of his head appeared to be cut off and his 3D CT scan confirmed the degree of flatness.
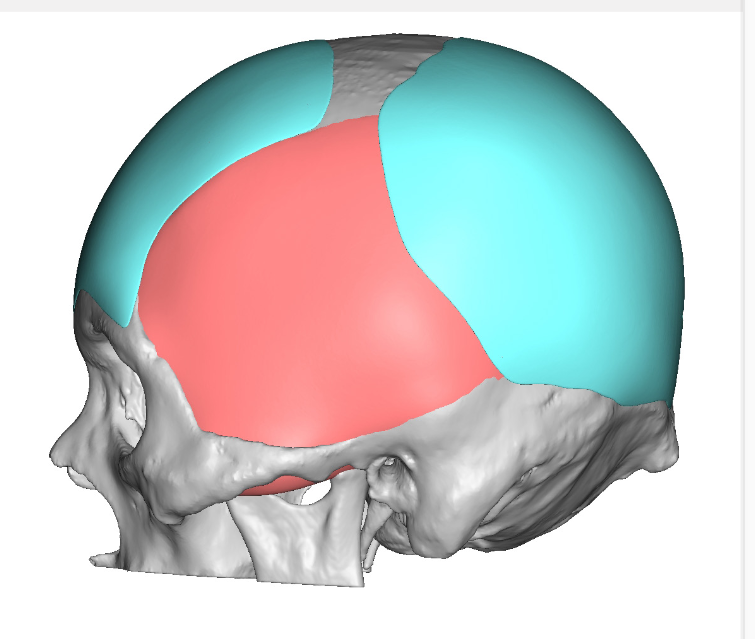
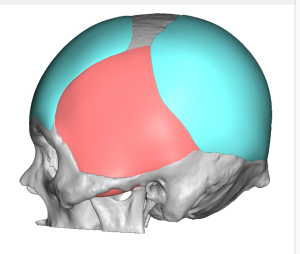 From his 3D CT scan a back of the implant was designed that provided 14mm projection and 140ccs of volume. A forehead implant was also designed of much less projection and volume.
From his 3D CT scan a back of the implant was designed that provided 14mm projection and 140ccs of volume. A forehead implant was also designed of much less projection and volume.


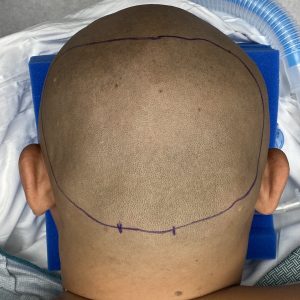
 Under general anesthesia and initially in the prone position a 7cm lower hirozontal scalp incision made over the occipital knob area of the back of the skull. Wide subperiosteal undermining over the entire back of the skull was performed to make the space for the implant. The implant, whose diameter was much wider than the incision, was rolled for insertion and then unrolled once inside the pocket. It was positioned and secured with 2.0mm titanium micro screws. A drain was placed prior to closure.
Under general anesthesia and initially in the prone position a 7cm lower hirozontal scalp incision made over the occipital knob area of the back of the skull. Wide subperiosteal undermining over the entire back of the skull was performed to make the space for the implant. The implant, whose diameter was much wider than the incision, was rolled for insertion and then unrolled once inside the pocket. It was positioned and secured with 2.0mm titanium micro screws. A drain was placed prior to closure.




He was then turned over for the custom forehead implant procedure.

 When seen the next day for his head dressing and drain removal the change in his skull length and shape was evident.
When seen the next day for his head dressing and drain removal the change in his skull length and shape was evident.
Case Highlights:
1) In certain ethnicities there is a tendency for underdevelopment of the skull in a anteroposterior direction
2) Custom skull implants can be designed to add projection to both the front and back of the skull to increase skull length.
3) Custom forehead and back of the head skull implants can be placed during the same surgery using different operative positioning.
Dr. Barry Eppley
Indianapolis, Indiana