

Background: Augmentation of the upper (forehead-brow bone) and lower (chin-jawline) third of the face have well known techniques, how to do so for the middle third of the face is less clear. What anatomically separates the middle third of the face for the upper and lower face is that is has a major concave component to it. The infraorbital rims and cheeks ideally have a convex shape to them, the maxilla and pyriform aperture regions of the lower midface are concave in shape.
Augmentation of the deficiency midface is historically done moving the midface bones forward by osteotomy. Various levels of LeFort osteotomies exist to treat lower to complete midface skeletal deficiencies. For total midface bony augmentation a LeFort III osteotomy would be needed. Understandably given the magnitude of the procedure and the changes that would occur at the tooth level this is not an appealing option for most patients.
Injection fat grafting is the most common form of midface augmentation today. While effective for some selective midface areas like the cheeks or undereyes, injecting fat for a more complete midface effect would undoubtably cause a bloated looking appearance that would be very hard if not impossible to reverse.
Implants remain a very useful method of midface augmentation. Standard cheek, pyriform aperture and tear trough implants can be useful for spot augmentations of the midface. But for a total midface effect no mixture of standard midface implants will work for an effective and complete augmentation result. This is where the role of custom midface implants comes into play.
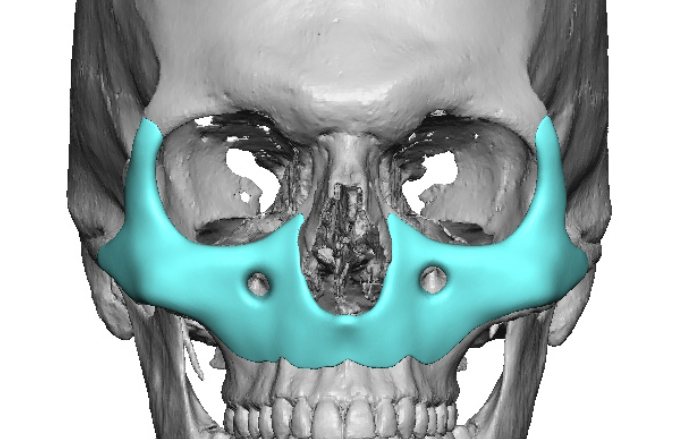
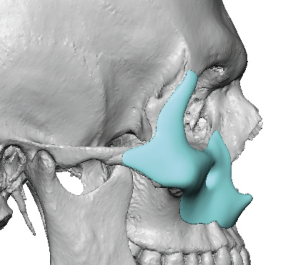 Case Study: This male wanted to have s complete midface augmentation done as he felt his midface was recessed. He had a good occlusion and chin projection. Using his 3D CT scan a custom midface implant was designed that augmented the midface from the lateral brow down to the low maxilla. Total implant volume was 11ccs.
Case Study: This male wanted to have s complete midface augmentation done as he felt his midface was recessed. He had a good occlusion and chin projection. Using his 3D CT scan a custom midface implant was designed that augmented the midface from the lateral brow down to the low maxilla. Total implant volume was 11ccs.
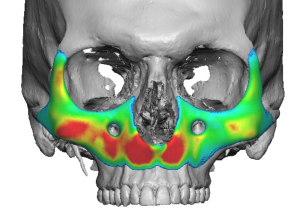 The greatest projection of the implant (4mms, red color) was around the pyriform aperture area where he had the greatest recession.
The greatest projection of the implant (4mms, red color) was around the pyriform aperture area where he had the greatest recession.


 Under general anesthesia and through an intraoral approach the entire midface was degloved up to the infraorbital rim and out onto the zygomatic arch. To get a good dissection up to the lateral brow area small lateral upper eyelid incisions were made for direct access to that remote area. The implant was prepared by placing multiple 4mm holes as well as enlarging the infraorbital nerve opening. The implant was introduced as a single piece, threading the lateral orbital rim portions up onto the lateral brows. Getting this thin implant area into proper position is the key to the whole placement of a complete or extended implant.
Under general anesthesia and through an intraoral approach the entire midface was degloved up to the infraorbital rim and out onto the zygomatic arch. To get a good dissection up to the lateral brow area small lateral upper eyelid incisions were made for direct access to that remote area. The implant was prepared by placing multiple 4mm holes as well as enlarging the infraorbital nerve opening. The implant was introduced as a single piece, threading the lateral orbital rim portions up onto the lateral brows. Getting this thin implant area into proper position is the key to the whole placement of a complete or extended implant.

 Once in proper position the implant was secured using four screws, two at the lateral orbital rim and and another two at the cheekbone area.
Once in proper position the implant was secured using four screws, two at the lateral orbital rim and and another two at the cheekbone area.
 Before incisional closure an alar cinch suture was placed to help narrow the nostrils. A V-Y musculomucosal closure was then done to bring back in the released midfacial soft tissues.
Before incisional closure an alar cinch suture was placed to help narrow the nostrils. A V-Y musculomucosal closure was then done to bring back in the released midfacial soft tissues.

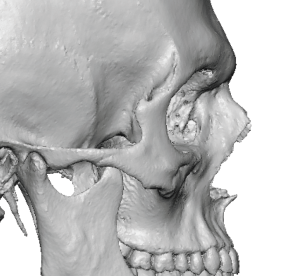
 The effects of the custom implant on midface projection could be appreciated in profile.
The effects of the custom implant on midface projection could be appreciated in profile.
Because the custom midface implant covers such a large surface area it does not need to be particularly thick in any one area. In fact the most common design error is to make it too thick. The goal is different than the indications for a true LeFort III osteotomy in which larger midface deficiencies are being treated. But just like any LeFort procedures in which the midfacial tissues are degloved/released which can lead to nostril widening. It is the same degloving that is needed for a complete midface implant so the same preventive maneuvers for nostril narrowing needs to be done.
Case Highlights:
1) Augmentation of the entire midface can be done by a custom implant design that has an effect similar to a Lefort III osteotomy…minus the dentoalveolar changes.
2) Custom midface implants can be placed through an intraoral approach which may need to be supplemented with eyelid incisions based on how far along the orbital rim and zygomatic arch the implant extends.
3) To prevent postoperative nostril widening after facial degloving and implant placement an alar cinch suture and V-Y incisional closures are needed.
4) Besides the swelling it will take 4 to 6 weeks after surgery for the normal movement off the upper lips and smile to return.
Dr. Barry Eppley
Indianapolis, Indiana