

Background: The shape of the head is determined by the interface between the exposed bony surfaces of the skull and the overlying temporal muscles on its sides. This creates five surfaces (four sides and a top) which influences the appearance of the head from 360 degree viewing angles. Because any one of these skull surfaces connects with any least three of the other surfaces the shape of one influences the shape of the others. A dramatic example of this interaction is seen in plagiocephaly the most well known skull shape deformity. (The flat side of the back of the head results in a similar but usually less flattening effect on the contralateral forehead)
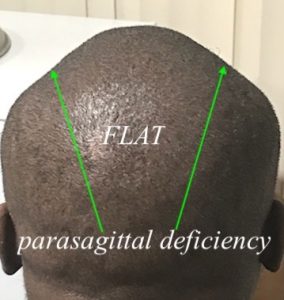
One underappreciated relationship of the skull surfaces is that of the temporal muscle. These bilateral non-bony sides of the skull do have an underlying bony component but the thick temporal muscles are far more responsible for what is seen on the outside. The origin of the temporal muscle is at the long raised bony temporal lines that run from the brow bones anteriorly to the back of the head. The location of the bony temporal on the sides of the head determines the length of the temporal muscle as well as the shape of the head as seen in the frontal view. The higher the bony temporal line the more convex or even more square head shape that results. The lower the bony temporal line the less convex and even V-shaped the head becomes.The low temporal line, which creates a steep or deficient parasagittal bone shape, can make the sagittal ridge appear raised. (pseudo sagittal crest head shape)
What happens to the temporal muscle when the bony temporal line is low? In many cases it is less in overall volume and the sides of the head simply become more narrow. But in outer cases, usually larger males with bigger overall skulls, the tenporal muscles bulge out as their volume is the same but they have less length one which to cover. This creates an abnormal transition between the top and sides of the head where a temporal muscle bulge occurs with a low almost V-shape groove along the bony temporal line. The apparent thickened upper portion of the temporal muscle could be reduced (not easily) or it can be covered over or augmented by a skull augmentation method that allows transitions over onto the upper portion of the temporal muscle. (more easily achieved) Which method is aesthetically best can be determined by preoperative imaging. But in the vertically short head an augmentation approach can be more effective.

 Case Study: This male desired a change in the shape of his head. He desired a smoother shape of his head in the front view and some augmentation to the back of his head. The nona-smooth transition of the bony skull to the muscle on the sides was very clear with bulging of the upper part of the temporal muscle and a lower temporal line.
Case Study: This male desired a change in the shape of his head. He desired a smoother shape of his head in the front view and some augmentation to the back of his head. The nona-smooth transition of the bony skull to the muscle on the sides was very clear with bulging of the upper part of the temporal muscle and a lower temporal line.
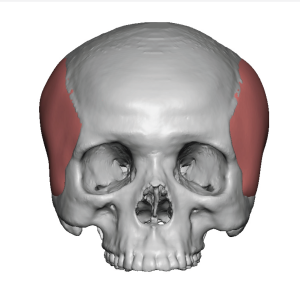
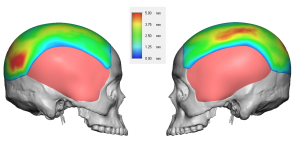
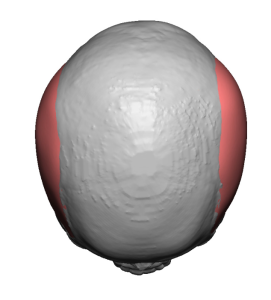 His 3D CT scan showed a short skull height with wide temples. The bony temporal line looked almost indented due to the muscle bulge along its sides.
His 3D CT scan showed a short skull height with wide temples. The bony temporal line looked almost indented due to the muscle bulge along its sides.
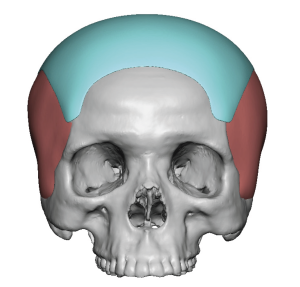
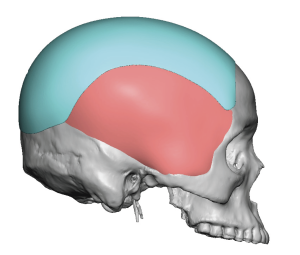
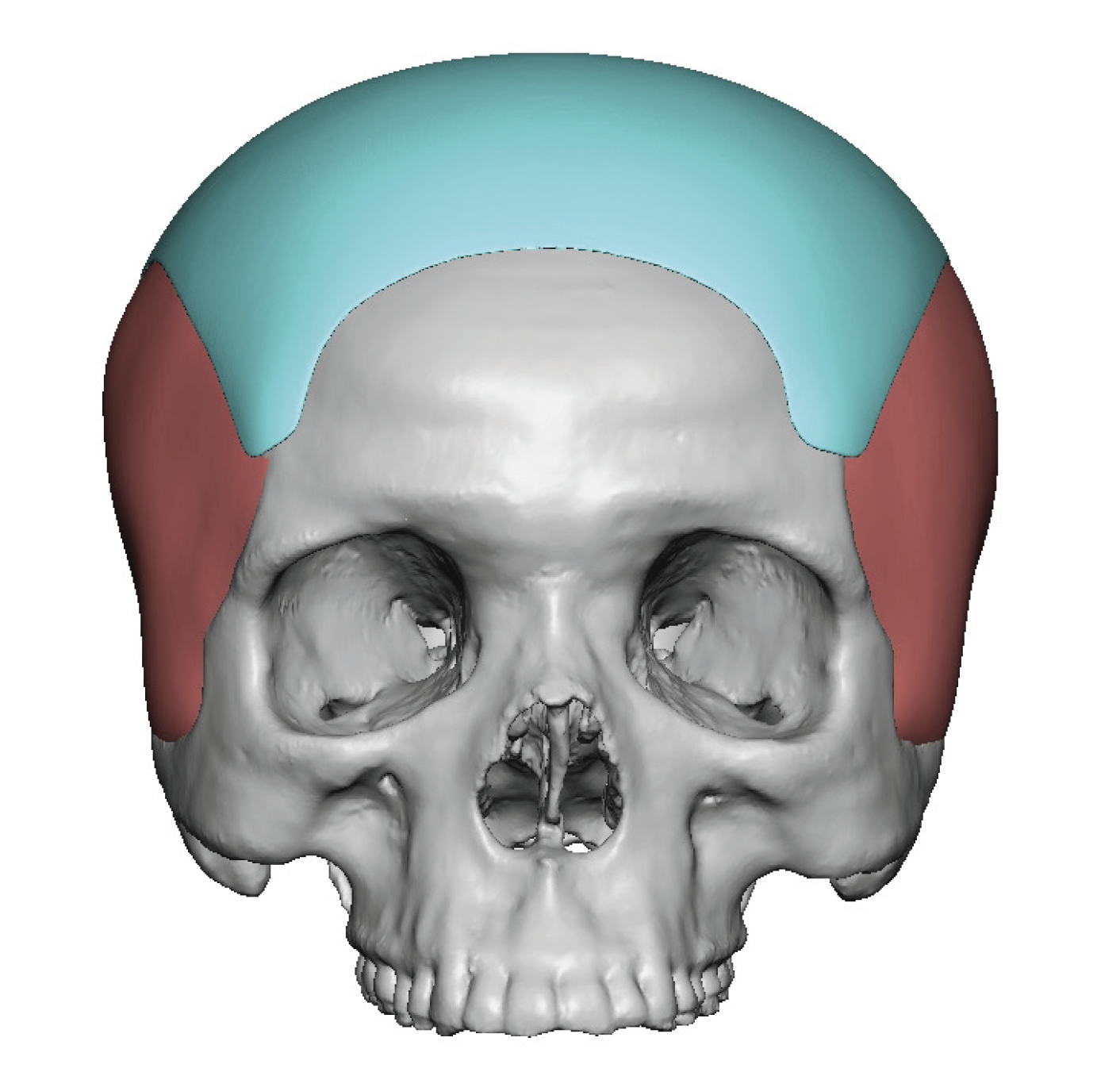
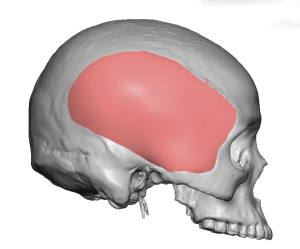
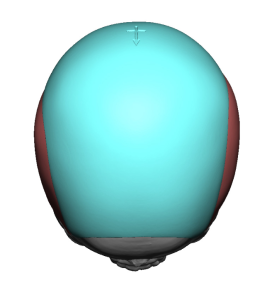 A custom skull implant was designed to cover the entire top of the head from the upper forehead all the way to the back down to the lambdoid suture line. The implant design extended beyond the bony temporal line onto the temporal muscles. The goal being to smooth over the transition between the sides and top of the head as well as give some added skull height. Total implant volume was 100ccs.
A custom skull implant was designed to cover the entire top of the head from the upper forehead all the way to the back down to the lambdoid suture line. The implant design extended beyond the bony temporal line onto the temporal muscles. The goal being to smooth over the transition between the sides and top of the head as well as give some added skull height. Total implant volume was 100ccs.
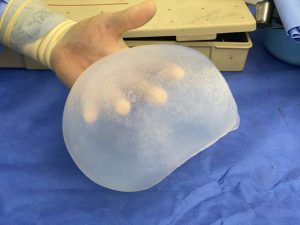
 Under general anesthesia and through a 9cm scalp incision placed anterior to the crown of the head wide subperiosteal undermining was done from the brow bones in front down to nuchal ridge in back. Dissection was carried onto the deep temporal fascia on the sides. Comparing the skull implant to the side of the incision showed quite a discrepancy.
Under general anesthesia and through a 9cm scalp incision placed anterior to the crown of the head wide subperiosteal undermining was done from the brow bones in front down to nuchal ridge in back. Dissection was carried onto the deep temporal fascia on the sides. Comparing the skull implant to the side of the incision showed quite a discrepancy.
Getting the implant through the incision relies on the deformability of the solid silicone material. While getting it through the incision is a feat onto itself, it is even more challenging to get it fully unfolded and then into proper position as per the design…without being able to visualize most of the implant.

 After placement and scalp incision closure the change in the shape of his head could be seen with a smoother convex shape.
After placement and scalp incision closure the change in the shape of his head could be seen with a smoother convex shape.
 In improving an abnormal head shape large areas of the skull usually need to be covered to achieve the effect. The surface area of coverage is often more important than any specific area of implant thickness. Going over onto the side of the head, as done in this case, may be needed and this poses some unique considerations. The augmentation needs to be on top of the muscle and never underneath it if a smooth contour is to be achieved across the bony temporal line. It takes a soft material that can be made with a fine edge to have smooth transition onto a soft tissue surface.
In improving an abnormal head shape large areas of the skull usually need to be covered to achieve the effect. The surface area of coverage is often more important than any specific area of implant thickness. Going over onto the side of the head, as done in this case, may be needed and this poses some unique considerations. The augmentation needs to be on top of the muscle and never underneath it if a smooth contour is to be achieved across the bony temporal line. It takes a soft material that can be made with a fine edge to have smooth transition onto a soft tissue surface.
Case Highlights:
1) The wide flat head shape can be associated with apparent thick temporal muscle protrusions due to a low bony temporal line.
2) A custom skull implant design can smooth out the transition between the temporal muscles and the bony skull on top to create a smoother head shape.
3) Placing a long relatively thin skull implant through a limited scalp incision poses challenges that requires experience and persistence to overcome.
Dr. Barry Eppley
Indianapolis, Indiana