

Background: Skull implant augmentation is a very successful strategy for flat or underdeveloped head shapes. In their most common use there is a single skull surface that is flat or non-rounded and a skull implant is designed to treat it. Such skull implants are placed in a single surgery as their aesthetic needs usually falls within the stretch of the scalp to accommodate it. But as skull implants become larger the consideration of how much the scalp can stretch to cover it takes on considerable importance. In essence, at what implant size will there not be enough scalp elasticity in which it can be successfully placed?
By extensive experience I have learned that skull implant volume is more important than any single area of implant thickness. While there is definitely a correlation between implant thicknesses and implant volume, what is very different about the desire for larger skull implant augmentations is their large surface area of coverage. As a result the footprint of the implant makes a major contribution to the volume of the implant that thickness alone does not suggest. The cutoff implant volume is around 150ccs for most patients to successfully place a single stage skull implant. Above this implant volume more scalp is needed and this is the role of a 1st stage scalp tissue expander in creating the sub-scalp space in which the implant can fit.
Besides making sure that enough scalp exists to cover large skull implants a second important consideration is how to get the implant placed with the smallest scalp incision as possible. While a bicoronal scalp incision will permit any size skull implant to be placed the vast majority of patients will not find this long scalp scar acceptable. As a result comparatively small scalp incision are used for all custom skull implants. While deformation of the implant will allow it to pass through these small scalp incisions this will not be so for larger skull implants. Rather than commit to making a long scalp incision the alternative strategy is to make the skull implant ‘smaller’ by a two piece design.
 Case Study: This female desired to have a substantial improvement in her head shape/size. The head area that needed the greatest volume increase was at the crown… which is typical for female large skull augmentations. A scalp tissue expander was initially inserted and she was able to successfully add 225cc in saline fluid volume to it.
Case Study: This female desired to have a substantial improvement in her head shape/size. The head area that needed the greatest volume increase was at the crown… which is typical for female large skull augmentations. A scalp tissue expander was initially inserted and she was able to successfully add 225cc in saline fluid volume to it.
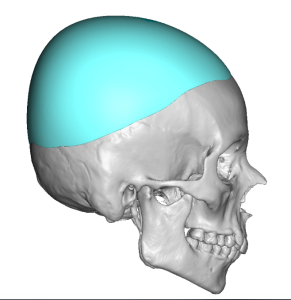
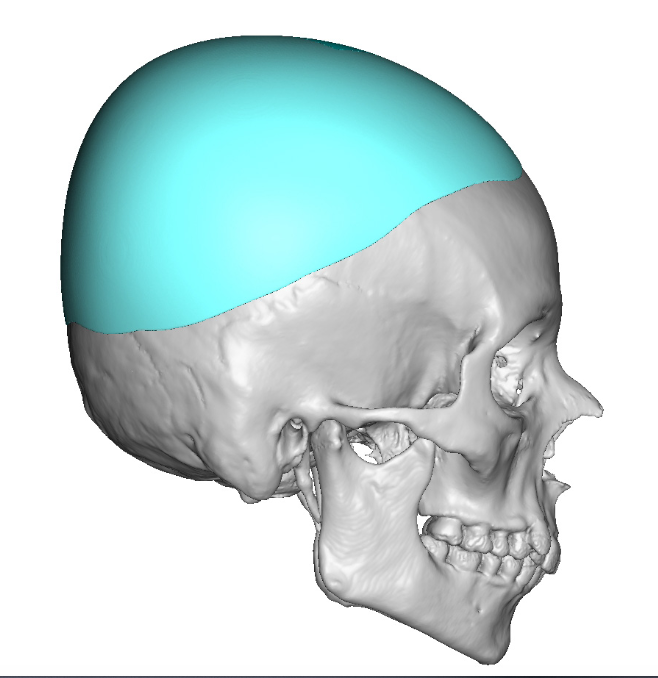
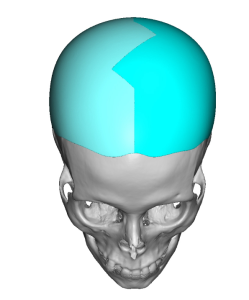 A scalp implant was designed whose footprint covered most of the skull’s surface within the hair-bearing scalp. Its total implant volume was 250ccs. A sagittal (midline) split design was done to aid in its insertion.
A scalp implant was designed whose footprint covered most of the skull’s surface within the hair-bearing scalp. Its total implant volume was 250ccs. A sagittal (midline) split design was done to aid in its insertion.
 Under general anesthesia and in the prone position the tissue expander was deflated and removed through the same inicision by which it was put in. A capsulectomy was preformed on the skull bone’s surface and a capsulotomy (release) was done around the perimeter of the expander’s capsule to enlarge it for the skull implant.
Under general anesthesia and in the prone position the tissue expander was deflated and removed through the same inicision by which it was put in. A capsulectomy was preformed on the skull bone’s surface and a capsulotomy (release) was done around the perimeter of the expander’s capsule to enlarge it for the skull implant.
 The skull implant was opened into the operative field and it could be seen as it was laid over the tissue expander how much bigger it was than the expander.
The skull implant was opened into the operative field and it could be seen as it was laid over the tissue expander how much bigger it was than the expander.
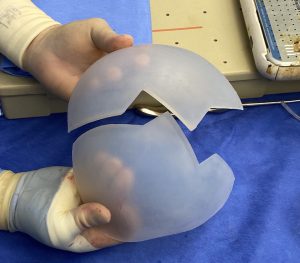
 Its geometric split design could be seen how it fits together which is important to know prior to attempting to place it.
Its geometric split design could be seen how it fits together which is important to know prior to attempting to place it.



 Without lengthening the existing scalp incision the skull implant was inserted right side at a time and then reassembled once under the scalp. It was secured by suture fixation between each side as well as secured to the bone by screws. Scalp closure was done by multilayer resorbable sutures.
Without lengthening the existing scalp incision the skull implant was inserted right side at a time and then reassembled once under the scalp. It was secured by suture fixation between each side as well as secured to the bone by screws. Scalp closure was done by multilayer resorbable sutures.

 The difference in the fullness of her head shape, even between the tissue expander and the skull implant, could be seen.
The difference in the fullness of her head shape, even between the tissue expander and the skull implant, could be seen.
Large skull implant augmentations are made possible by custom implant designs which ensure the exact surface area coverage, thicknesses, as well as a smooth contour on its outer surface. This is aesthetically far superior to the use of bone cements for skull augmentations which can ensure none of these three important characteristics. But a large premade skull implant must take into consideration of whether not will fit under the scalp as well as how to get it into the tissue pocket with the least amount of scalp scarring. As seen in this patient a 1st stage scalp expansion and a split implant design enable these limitations to be overcome.
Case Highlights:
1) Large skull implant augmentations requite a 1st stage expansion.
2) The amount of scalp expansion volume should match that of the custom skull implant’s design volume.
3) Surgical placement of large skull implants to keep the scalp incision as small as possible must be designed in at least two pieces.
Dr. Barry Eppley
Indianapolis, Indiana