

Background: The skull is affected by a variety of synostotic and deformational deformities that result in noticeable flat areas. The most well known of these flat head areas is plagiocephaly where its most significant effect is seen as a flat side of the back of the head. When more complete flatness occurs on the back of the head it is known as brachycephaly. While it can occur from bilateral lambdoid craniosynostosis it is far more commonly seen as a result of deformational forces (laying on the back of the head as an infant) particularly in those patients more predisposed to decreased anteroposterior skull growth.
In brachycephaly it is important to recognize that as the skull lacks projection the overlying scalp will be tighter than normal…as it also lacks projection/development. Thus when designing a custom skull implant to augment it there is going to be limits as to how much augmentation can be achieved. (i.e., will the implant fit) Considerable experience has shown these scalp stretch limits can be predicted by implant augmentation volume. As a general rule implant volumes under 150cc can be safely placed while those greater than 150cc are going to need some ‘help’.
This ‘help’ is in the form of a scalp tissue expander whose effect is similar to pregnancy. Through an initial placement of an expander device, it is slowly inflated over several months to reach the same volume as that of the designed skull implant. This is a process that takes close to 3 months to be fully achieved.
Case Study: This adult male desired to augment a very flat back of his head. Being Caucasian and with a fair complexion his scalp stretch was going to be very limited, probably barely enough to tolerate a 100cc implant. Such an augmentation result would have been barely worth it.

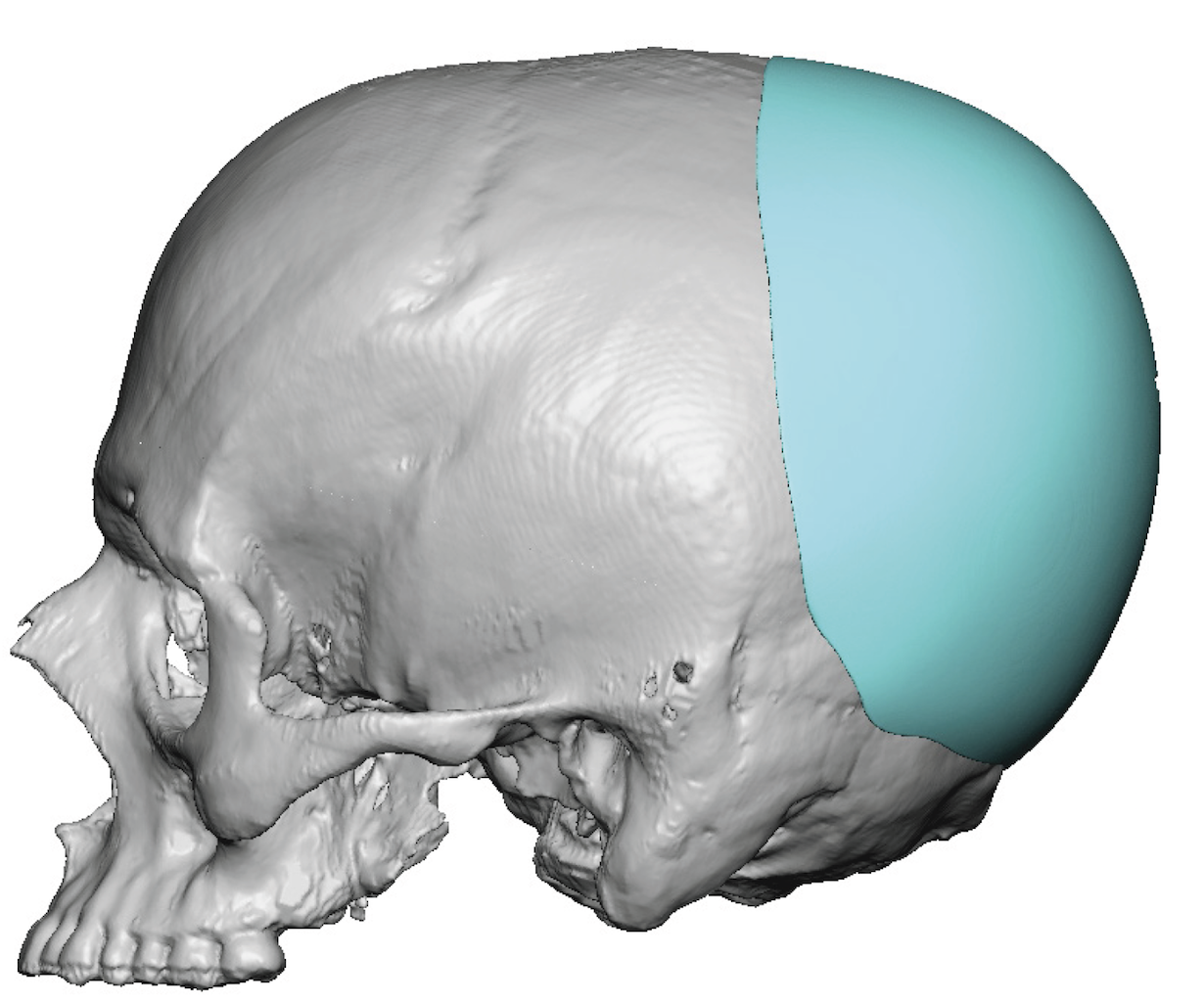
 Using computer imaging to determine the desired back of the head shape a custom skull implant was designed of 190cc volume. Its maximal thickness and point of projection was directly horizontal.
Using computer imaging to determine the desired back of the head shape a custom skull implant was designed of 190cc volume. Its maximal thickness and point of projection was directly horizontal.

 As a result a scalp expander was initially placed through a small incision on the back of the head. Over the next three months, adding 10ml volumes every 2 too 3 days he successfully reached a 190cc expander fill.
As a result a scalp expander was initially placed through a small incision on the back of the head. Over the next three months, adding 10ml volumes every 2 too 3 days he successfully reached a 190cc expander fill.
 Three months later the scalp tissue expander was removed, total capsule removal on the bone and capsulotomies around the edge of the expanded scalp allowed the large custom skull implant to be satisfactorily placed without undue incisional closure.
Three months later the scalp tissue expander was removed, total capsule removal on the bone and capsulotomies around the edge of the expanded scalp allowed the large custom skull implant to be satisfactorily placed without undue incisional closure.

 The immediate intraoperative result showed a back of the head augmentation effect that would have never been possible with0ut a prior scalp expansion.
The immediate intraoperative result showed a back of the head augmentation effect that would have never been possible with0ut a prior scalp expansion.
Custom skull implant designs allow virtually any size augmentation to be created. But the limitation is in how much can the scalp safely be pushed outward from an implant on the bone. While any form of aesthetic face and body implant augmentations can face a similar soft tissue limitation the scalp is unique because it is naturally tighter and a significant portion of it has hair follicles. Too aggressive immediate scalp expansion from an implant can potentially cause hair loss, temporary shock or even permanent follicle injury. Thus it pays to be cautious.
While no one really wants a two stage skull augmentation, getting satisfactory results in some patients with larger implant needs may make it necessary
Case Highlights:
1) Back of the head flatness is the most common aesthetic skull deficiency seen.
2) Brachycephaly is a complete flatness of the back of the head which is optimally treated by a custom designed skull implant whose projection depends on how much augmentation is desired.
3) If a large skull implant augmentation is desired a first stage scalp expander will be needed for a two stage skull augmentation procedure.