


Background: While often not appreciated correction of a narrow head width can be achieved today by various custom implant designs. But the term ‘head widening’ is a general one and must be qualified for each patient as to exactly what that means. There are two basic types of head widening requests…those that look to achieve an increased head width that does not involve the forehead and those that include the forehead. (does the implant need to cross the temporal line) That distinction is critically important in implant design and in surgical placement.
For the sake of simplicity I will call head widening that stays within the bony temporal line a Type 1 head widening implant (Type 1) and those that need to cross the temporal line as an extended or Type 2 head widening implant. The difference between the two surgically is their pocket location. The Type 1 head widening implants is placed in the submuscular pocket while the Type 2 head widening implant must be placed more superficially on top of the muscle (technically on top of the deep temporal fascia) so there can be a seamless transition in the contour of the augmentation from the forehead to the temples.
In either type of head widening implant the main site of insertion is done from the crease on the back side of the ear. (postauricular sulcus) In a Type 1 head widening implant that is the only incision needed. In Type 2 head widening implants an additional small incision is placed in the high temporal area near the side of the forehead to aid placement onto the forehead as well as provide a location for screw fixation to the bone.
 Case Study: This male was undergoing a three level facial augmentation procedure one of which was a Type 2 head widening. His 3D CT scan did not show an abnormally narrow head shape. But the intent was that as he was widening is lower face it made proportionate sense to widen the upper face as well.
Case Study: This male was undergoing a three level facial augmentation procedure one of which was a Type 2 head widening. His 3D CT scan did not show an abnormally narrow head shape. But the intent was that as he was widening is lower face it made proportionate sense to widen the upper face as well.
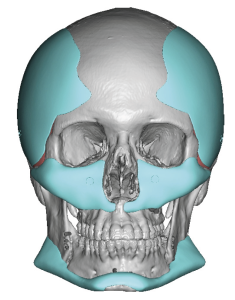
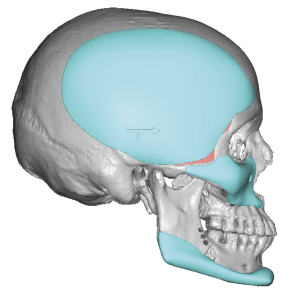 Using this 3D CT scan bilateral Type 2 head widening implants were designed that crossed onto the bony forehead. The maximum width thickness was 5mms and each implant side had a volume of 30ccs…which translates to a modest augmentation effect.
Using this 3D CT scan bilateral Type 2 head widening implants were designed that crossed onto the bony forehead. The maximum width thickness was 5mms and each implant side had a volume of 30ccs…which translates to a modest augmentation effect.

 Under general anesthesia the outline of the implants onto his forehead and temporal areas was marked.
Under general anesthesia the outline of the implants onto his forehead and temporal areas was marked.
 The posterior placement of the implants could be seen by laying the implants onto the outer temporal area.
The posterior placement of the implants could be seen by laying the implants onto the outer temporal area.
 Through postauricular incisions the implant pockets were developed on top of the deep temporal fascia onto the bony forehead. This was aided by a small incision right behind the frontotemporal hairline. The implants were inserted through the incisions, positioned as per the design and secured with a microscrew to the upper bony forehead and to the temporal bone through each incision site.
Through postauricular incisions the implant pockets were developed on top of the deep temporal fascia onto the bony forehead. This was aided by a small incision right behind the frontotemporal hairline. The implants were inserted through the incisions, positioned as per the design and secured with a microscrew to the upper bony forehead and to the temporal bone through each incision site.
For head widening the traditional craniofacial approach is to think of bone augmentation. But the thickness of the side of the head is made up as much about muscle as it is bone. As a result isolated side of the head widening involves muscle augmentation typically done by submuscular implant augmentation. (which may also be seen as expanding the bone contour under the muscle) But when the side of the head augmentation requires forehead widening as well a bone augmentation approach will not work as it cannot effectively cross the bony temporal line without disrupting the muscle attachments. (which will cause a contour problem) As a result the augmentation must be done on top of the muscle so a smooth augmented contour can extend onto the side of the forehead. This poses its own potential issues (implant edging, fluid collections) that do not exist with pure submuscular temporal implant augmentation but these can be avoided/overcome by implant design/placement techniques.
Key Points:
1) It is important in head widening to determine if it needs to extend onto the sides of the forehead to not.
2) Head widening that extends onto the forehead must be done on top of the deep temporal fascia for a smooth contour around the side of the head.
3) Custom extended temporal implants can be placed through postauricular incisions.
Dr. Barry Eppley
World-Renowned Plastic Surgeon