


Hip implants are unique amongst all aesthetic body implants. Their vertical orientation in a more superficial tissue pocket location is what separates it from other body implants. Any extremity (arm and leg) implant does also have a periodic vertical orientation but those implants are either in the subfascial or submuscular pockets which provide better implant camouflage and support. The hip implant, however, is on top of the muscle fascia (deep subcutaneous layer) where the soft tissue cover is less and the subcutaneous fat layer provides less implant support.
As a result the hip implant can develop some unique postoperative aesthetic issues which can occur at its lower half. (implant edge visibility) One reasons is an implant buckle or fold at the very thin lower edge. Since is is a vertically oriented implant and it has a feathered edge at the bottom the weight of the implant can cause its bottom third to bend or buckle) which appears as an external visible bulge Another reason for edging is inadequate pocket dissection. The implant simply doesn’t have enough space to fully lay out. Lastly the bottom edge of the dissection may have ended up stickling into the subcutaneous fat layer as opposed to laying flat on the fascia.
 Having seen all three types of hip implant edge visibility the bottom edge of the implant sticking up into the subcutaneous tissue is the easiest to diagnose by look and feel. If it occurs the corrective treatment is to make a small incision inferiorly and get the implant better positioned on the fascia. The other reasons are harder to diagnose but their treatment is the same…release of the capsule. (pocket expansion)
Having seen all three types of hip implant edge visibility the bottom edge of the implant sticking up into the subcutaneous tissue is the easiest to diagnose by look and feel. If it occurs the corrective treatment is to make a small incision inferiorly and get the implant better positioned on the fascia. The other reasons are harder to diagnose but their treatment is the same…release of the capsule. (pocket expansion)

 While inferior implant edging by release can be treated by an open incisional approach, and the scar that it will leave is not terrible, it would certainly be nice to avoid it. In that regard an alternative approach is a percutaneous technique. This can be done under local anesthesia using 18 gauge needles.
While inferior implant edging by release can be treated by an open incisional approach, and the scar that it will leave is not terrible, it would certainly be nice to avoid it. In that regard an alternative approach is a percutaneous technique. This can be done under local anesthesia using 18 gauge needles.


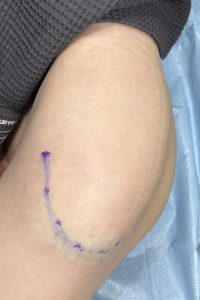
 The bevel on an 18 gauge needle is much like a small scalpel. Entering at numerous puncture points along the line of the implant edge tiger capsule is incised. The objective is to make the release complete along the entire marked line by moving the bevel of the needle back and forth at each entrance point. The implant and capsule can be felt with the needle.
The bevel on an 18 gauge needle is much like a small scalpel. Entering at numerous puncture points along the line of the implant edge tiger capsule is incised. The objective is to make the release complete along the entire marked line by moving the bevel of the needle back and forth at each entrance point. The implant and capsule can be felt with the needle.
There will be some minor bleeding through the needle entrance sites as would be expected from the cutting action along the capsular tissues The needle entrance sites will not leave any visible scars. There is no need for any post procedure dressings or limitation of activity. The question then becomes how effective will it be. If the diagnosis is correct the implant edging should be reduced. At the least it is a minimally invasive procedure to try before committing an open approach with a small scar.
the implant edging should be reduced. At the least it is a minimally invasive procedure to try before committing an open approach with a small scar.
Dr. Barry Eppley
World-Renowned Plastic Surgeon