

Background: The use of an implant is the most common form of chin augmentation. It offers a predictable method of bone augmentation based on the thickness of the implant. But the placement of an implant requires that the soft tissue chin pad be released and an implant placed as an interface between the bone and the soft tissue chin pad. As a result there are limitations of how much implant material can be tolerated between the two. This is why almost all chin implants are 10 mm or less in projection as well as most patients need less than that amount of augmentation for a good aesthetic outcome.
But in more severely recessed chins an implant is going to be insufficient. Besides the need for more than 10 mm of horizontal projection the chin is often tilted backwards and elongated in which the placement of an implant in advertently loses some of the horizontal horizontal augmentation and can add undesired vertical length. This is where the role of the sliding genioplasty is indicated. Besides being able to add greater amounts of horizontal augmentation that an implant it also can bring the chin forward to either maintain its current vertical lengthen it or even shorten it.
It is not uncommon in severely recess chins to see a patient who’s had an initial chin implant with an inadequate result. This often occurs because the patient is not willing to undergo an initial sliding gemioplasty and preferred a less invasive surgery or the surgeon only offered an implant as a treatment option. This raises an interesting question as to whether remove the implant and perform a maximum sliding genioplasty or retain the implant and move the bone forward with the implant attached. Which approached is advised depends on the total amount of horizontal chin augmentation that is ideally needed as well as the position of the existing implant on the bone.
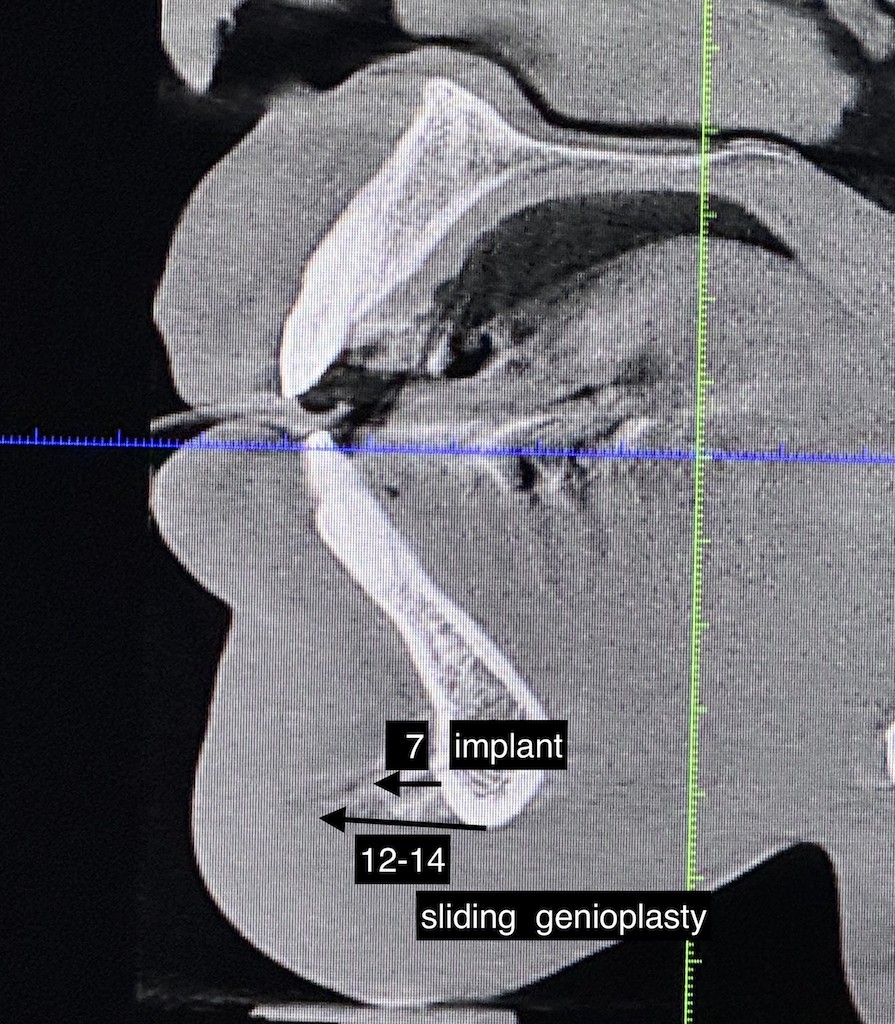
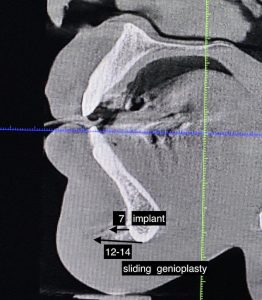 Case Study: This male had a history of a prior chin implant which he felt provided some improvement but was still short of his ideal augmentation goal. His chin implant had been placed using an intraoral approach, was positioned low on the bone and had three long screws for fixation. By measurements the chin implant provided 7 mm of horizontal projection. By external measurements he needed another 10 to 12 mm of horizontal chin augmentation to bring his chin out close to a vertical line dropped down from the lower lip. The recessed chin could be seen to be tilted backwards with adequate vertical length. As a result any additional horizontal chin augmentation must ensure that no additional vertical length was added or, more ideally, even shorten the chin in a bit.
Case Study: This male had a history of a prior chin implant which he felt provided some improvement but was still short of his ideal augmentation goal. His chin implant had been placed using an intraoral approach, was positioned low on the bone and had three long screws for fixation. By measurements the chin implant provided 7 mm of horizontal projection. By external measurements he needed another 10 to 12 mm of horizontal chin augmentation to bring his chin out close to a vertical line dropped down from the lower lip. The recessed chin could be seen to be tilted backwards with adequate vertical length. As a result any additional horizontal chin augmentation must ensure that no additional vertical length was added or, more ideally, even shorten the chin in a bit.

 Under general anesthesia and through an intraoral approach the chin implant was exposed and seen to be in very stable position. (it was slightly off center to the left) Using a reciprocating saw a full thickness bone cut was made along the top of the implant and the bone with the implant was down fractured. Using a 12mm step plate the chin bone with implant was advanced and secured with screws into its new position. The plate was bent with an upward tilt to prevent any additional chin lengthening.
Under general anesthesia and through an intraoral approach the chin implant was exposed and seen to be in very stable position. (it was slightly off center to the left) Using a reciprocating saw a full thickness bone cut was made along the top of the implant and the bone with the implant was down fractured. Using a 12mm step plate the chin bone with implant was advanced and secured with screws into its new position. The plate was bent with an upward tilt to prevent any additional chin lengthening.

 After the application of dehydrated cadaveric bone chips into the step deformity the intraoral incision was closed in multiple layers with resorbable sutures. The side profile shows the improvement in chin projection with the additional 12mm advancement.
After the application of dehydrated cadaveric bone chips into the step deformity the intraoral incision was closed in multiple layers with resorbable sutures. The side profile shows the improvement in chin projection with the additional 12mm advancement.
In this inadvertent two stage chin augmentation the patient ended up with a greater amount of chin augmentation than if either approach had been done alone. (18mms +horizontal advancement) When patients need very large chin augmentations it is because their lower jaw is underdeveloped and the problem is greater than just a short chin. ideally they need a combined jaw advancement and chin augmentation to reach their ideal augmentation goals. But if not going through that approach then it requires a maximum chin augmentation technique.
A sliding genioplasty can be done with a chin implant in place IF the chin placement is low enough on the bone that an osteotomy cut can be safely done above it. In many cases this can not be done as the chin implant placement is too high or the chin implant is tilted so that the side wings are angled up too high..
Key Points:
1) The sliding genioplasty offers greater horizontal chin advancements than that of an implant.
2) When performing a sliding genioplasty after a chin implant the implant can be retained with the bone movement if it is positioned low enough and is securing screwed into position.
3) Most secondary sliding genioplasties are going to be limited to 10 to 12 mm of bone movement with the retention of the chin implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon