


Background: Excessive projection on the back of the head is a common request for skull reduction. Consideration for whether such skull reduction can be a good aesthetic procedure is how much reduction can be achieved and where is the incisional access going to be to do it. The effectiveness of the procedure depends on how much bone can be safely removed which requires a preoperative x-ray to determine. I used to use a plain lateral skill film to do so but a 2D CT scan provides a more in depth assessment.
When considering occipital skull reduction whether a superior or inferior approach is used depends on the location of the maximal area of projection. By far the most common approach is an inferior one with a low scalp incision over the nuchal ridge. But there are indications for a superior approach of the greatest projection is on the upper end of the bone. While the thickest part of the occipital bone is at the knob or inion area, and this usually creates the area of greatest projection, it can also occur at its upper end at the lambdoidal suture line.

 Case Study: This young male was bothered by a back of the head protrusion of which its greater prominence was at the upper half of the occipital bone. Through a superior zigzag incisional approach the occipital prominence was reduced just shy of the diploid space.
Case Study: This young male was bothered by a back of the head protrusion of which its greater prominence was at the upper half of the occipital bone. Through a superior zigzag incisional approach the occipital prominence was reduced just shy of the diploid space.

 Closure of the scalp incision was done in multiple layers over a drain with resorbable sutures.
Closure of the scalp incision was done in multiple layers over a drain with resorbable sutures.

 He was seen four years later for other procedures in which the long term results from the reduction in the back of his head could be seen.
He was seen four years later for other procedures in which the long term results from the reduction in the back of his head could be seen.
 His scalp incision had healed so well that it could not be found even on close inspection.
His scalp incision had healed so well that it could not be found even on close inspection.
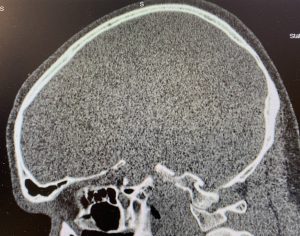 A postoperative CT scan shows the thinned occipital bone above the occipital knob area.
A postoperative CT scan shows the thinned occipital bone above the occipital knob area.
The occipital bone occupies the lower half of the back of the head and is separated from the parietal bones by the lambdoid suture line. In most occipital bun deformities the bone raises up above the suture line and creates a noticeable step off to the elevated protrusion. This is very evident from a superior approach and is most readily reduced from that direction. When approaching the occipital bun inferiorly there is no suture line and only a bulge is seen. Which incisional approach should be used for the bun depends on what the patient sees as the most important area of reduction needed.
Key Points:
1) Occipital bone reduction can be done from an inferior or superior approach which slightly different aesthetic outcomes.
2) A superior back of head incision heals well in an inconspicuous manner.
3) If the bone is thick enough an effective skull reduction on the back of the head can be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon