

Frontal bossing is a well-recognized aesthetic skull deformity that can present in various forms. It manifests as a prominent forehead or an overall convex forehead shape, often accentuated by a high or receded frontal hairline. In many cases, the increased distance between the eyebrows and the hairline amplifies the appearance of the forehead prominence.
Anatomy and Development of the Frontal Bone
A clear understanding of frontal bossing begins with the anatomy of the frontal bone. This single, large bone forms the forehead and extends over the top of the skull. Anatomically, it has two parts:
-
The lower horizontal component, which forms the roof of the orbits (brow bones).
-
The vertical component, which creates the forehead.
Although these subunits are not visible externally, they are crucial in understanding the mechanics of frontal bossing.
Embryologically, the frontal bone originates from two ossification centers, one on each side of the frontal suture. As the bone matures, these centers fuse across the metopic suture to form a single, continuous bone. Residual prominence of these ossification centers can result in minor forms of bossing, such as forehead horns. More pronounced bossing is typically due to overdevelopment of the vertical component of the frontal bone, while the horizontal (brow bone) component remains normally developed.
Key Considerations in Treatment
When treating bony forehead prominences, two main factors must be considered:
-
The maximum amount of frontal bone that can be safely reduced.
-
The location and length of the scalp incision required to adequately expose the bone.
Case Study
This male patient presented with multiple skull shape concerns, including:
-
Frontal bossing.
-
A midline sagittal peak.
-
Bilateral parietal eminences.

 A 3D CT scan confirmed an overly convex frontal contour and a sagittal peak at the junction of the frontal bone and coronal suture.
A 3D CT scan confirmed an overly convex frontal contour and a sagittal peak at the junction of the frontal bone and coronal suture.
Surgical Approach
The patient prioritized the reduction of frontal bossing and, despite the aesthetic implications of a long scalp scar on his shaved head, preferred a fine-line scar over his forehead deformity. The same incision also allowed access for reducing the parietal eminences.
-
 Anesthesia and Exposure: Under general anesthesia, a near-coronal scalp incision was made. The frontal bone was exposed from the coronal suture down to the brow bones.
Anesthesia and Exposure: Under general anesthesia, a near-coronal scalp incision was made. The frontal bone was exposed from the coronal suture down to the brow bones. -
Bone Reduction: Using a high-speed handpiece and burr, the frontal bone was carefully reduced to the point of spot bleeding at the diploic space, signaling the safe limit of reduction. Bone bleeders were controlled with bone wax.
-
Parietal Reduction: The posterior scalp flaps were elevated to access the parietal eminences. The overlying temporal muscle and fascia were removed, and the bones were similarly reduced with a high-speed burr.
-
Closure: The scalp was closed over drains with small resorbable sutures.

 Anesthesia and Exposure: Under general anesthesia, a near-coronal scalp incision was made. The frontal bone was exposed from the coronal suture down to the brow bones.
Anesthesia and Exposure: Under general anesthesia, a near-coronal scalp incision was made. The frontal bone was exposed from the coronal suture down to the brow bones.
 Bone Reduction: Using a high-speed handpiece and burr, the frontal bone was carefully reduced to the point of spot bleeding at the diploic space, signaling the safe limit of reduction. Bone bleeders were controlled with bone wax.
Bone Reduction: Using a high-speed handpiece and burr, the frontal bone was carefully reduced to the point of spot bleeding at the diploic space, signaling the safe limit of reduction. Bone bleeders were controlled with bone wax.
 Parietal Reduction: The posterior scalp flaps were elevated to access the parietal eminences. The overlying temporal muscle and fascia were removed, and the bones were similarly reduced with a high-speed burr.
Parietal Reduction: The posterior scalp flaps were elevated to access the parietal eminences. The overlying temporal muscle and fascia were removed, and the bones were similarly reduced with a high-speed burr.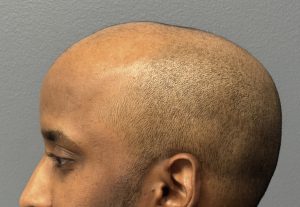
 Drains were removed two days later. Early results showed a visibly reduced forehead contour, with final results expected within 2–3 months.
Drains were removed two days later. Early results showed a visibly reduced forehead contour, with final results expected within 2–3 months.
Technical Insights
While bony reduction can be performed on any skull surface, the thickness of each area dictates how much reduction is possible:
-
Occipital bone (back of head): Thickest, at 10mm or more.
-
Temporal bone: Thinnest, at 5mm or less.
-
Parietal and frontal bones: Intermediate thickness, 6–10mm.
In men, the average frontal bone thickness is about 8mm—sufficient to allow a noticeable reduction in forehead prominence, provided bone thickness is within normal limits as confirmed by CT imaging.
Key Takeaways
? Frontal bossing presents in varying degrees, from subtle forehead horns to complete overgrowth of the frontal bone.
? A near-coronal scalp incision is often required to achieve complete and satisfactory bone reduction.
? Preoperative CT scan assessment is essential to evaluate the frontal bone thickness and determine the safe extent of reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon