

Does the weight and size of the patient affect healing of clavicle bone surgeryu?
Yes—patient size and weight can meaningfully influence healing after clavicle bone surgery, but not always in a simple “heavier = worse” way. It’s more about the physiologic and mechanical effects that often come along with higher body weight or larger body habitus.
Here’s how it breaks down:
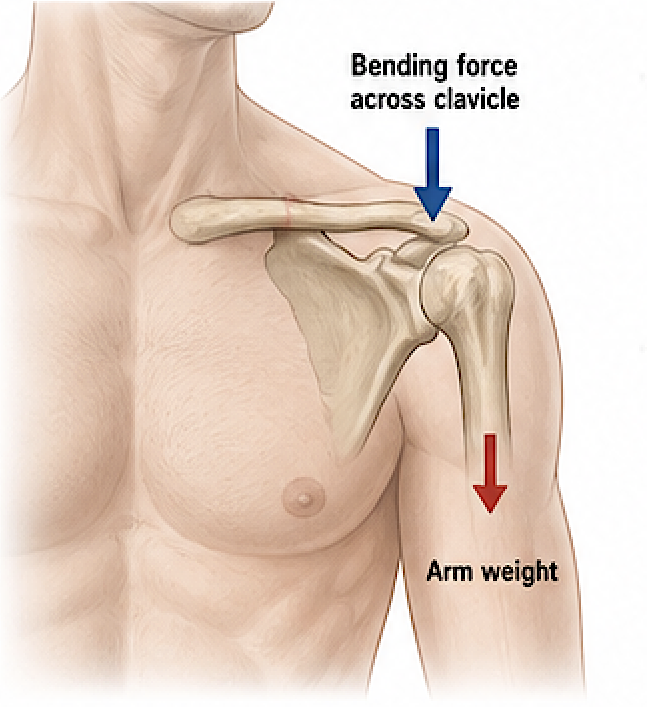
1. Mechanical load on the clavicle
- The clavicle acts as a strut supporting the shoulder.
- Larger patients (especially with more upper body mass) place greater forces across the osteotomy site.
- This can increase risk of:
- delayed union
- hardware fatigue or failure (plates/screws)
- loss of correction
2. Soft tissue thickness
- Heavier patients typically have thicker soft tissue over the clavicle.
- This can:
- reduce prominence/irritation of hardware (a benefit)
- but also make surgery more technically demanding and slightly increase risk of wound complications (e.g., seroma, infection)
3. Biological healing factors
Weight itself isn’t the direct issue—associated conditions matter more:
- Obesity is often linked with:
- lower-grade chronic inflammation
- impaired microcirculation
- insulin resistance or diabetes
- These can slow bone healing and increase infection risk.
4. Bone quality
- Not strictly tied to weight, but:
- very low body weight ? potential for poorer bone density
- obesity doesn’t guarantee good bone quality
- Bone density affects how well fixation holds and how quickly union occurs.
5. Activity level and compliance
- Larger patients may have more difficulty with postoperative restrictions (e.g., limiting arm use), which can stress the osteotomy.
- Conversely, very thin patients may have less mechanical stress but more hardware irritation.
General takeaway
- Yes, body size matters, but mostly through:
- mechanical loading
- metabolic health (diabetes, inflammation)
- soft tissue characteristics
- A healthy, metabolically normal heavier patient may heal just fine.
- A patient with obesity plus diabetes or poor compliance has a higher risk of complications than weight alone would suggest.
As this relates to cosmetic clavicle shortening osteotomies in otherwise normal bone:
? Mechanical considerations (more important here)
- You are intentionally reducing clavicle length, which:
- decreases the strut function
- changes scapular positioning and shoulder biomechanics
- In larger/heavier patients, this matters more because:
- greater shoulder girdle mass ? higher bending forces across a shortened clavicle
- increased stress on fixation (plates/screws)
? Net effect:
- Higher risk of:
- delayed union or nonunion
- hardware fatigue/failure
- loss of intended shortening (creep or deformation)
Biological factors
- Usually these patients are healthy, so biology is favorable.
- But if obesity is present:
- subtle impairment in bone healing can still matter because this is a purely elective construct—there’s no biologic “drive” like fracture healing.
? Risk tolerance (critical difference)
- Cosmetic cases have zero functional necessity.
- Even small complication rates matter more.
- In a heavier patient, the threshold for concern is lower because:
- the mechanical disadvantage is self-created (shortening)
- complications are less acceptable
Bottom line for cosmetic cases
- Weight/size has a disproportionately negative effect
- Particularly important when:
- shortening is larger (>1.5–2 cm)
- patient has broad shoulders or high upper body mass
- Fixation strategy (strong plating, dual plating) becomes more important
Dr Barry Eppley
Plastic Surgery