

Custom deltoid implants can be considered for visible deltoid/shoulder hollowing after shoulder replacement, but they are contour-restoration devices, not functional muscle replacements.
Key points:
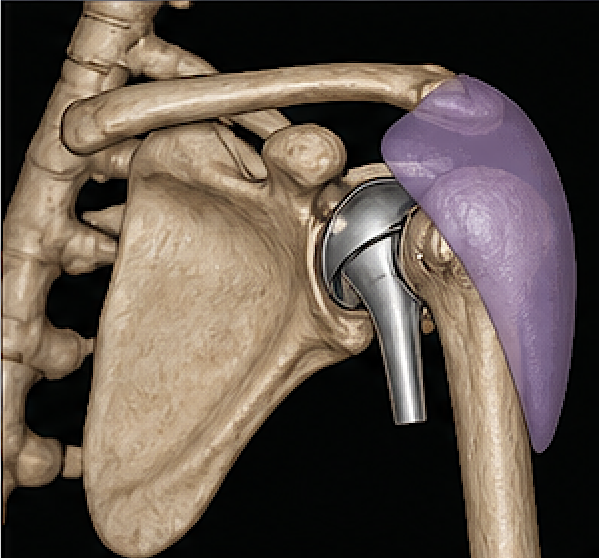
- After reverse shoulder arthroplasty, deltoid quality matters because the deltoid becomes the main elevator of the arm. Deltoid atrophy or nerve injury can affect function.
- A solid silicone custom deltoid implant may help restore the rounded shoulder contour when the atrophy is stable and localized. This is mainly aesthetic/symmetry reconstruction.
- It will not restore deltoid strength if the muscle/axillary nerve is deficient.
- With a prior shoulder arthroplasty, the major added concerns are:
- proximity to prosthetic hardware
- infection risk
- scarred surgical planes
- need to avoid deltoid compromise
- confirming the shoulder replacement is stable and not infected
For a post-arthroplasty patient, I’d generally favor a custom low-profile deltoid contour implant placed superficial to the deltoid/fascial plane, designed to camouflage the hollow without interfering with the shoulder prosthesis. But when only a thin soft tissue cover lies over the incision line direct implant placement underneath it is not advised. Soft tissue volume restrodation is needed by fat grafting. Dermal-fat grafting is needed to create increased soft tissue thickness, particularly at the anterior deltoid-pectoral junction prior the placement of the implant. This is a superior approach to fat injections in effectiveness.
Case Example

 This older male wanted deltoid implants to help restoire lost muscle mass after having had 3 shoulder replacement surgeries. A long surgical scar eexisted anteriorly over the deltoid-pectoral junction. The left side was deeper (more tissue deficient) than that of the right, Before proceeding with deltoid implants soft tissue volume restoration over the scar lines was needed.
This older male wanted deltoid implants to help restoire lost muscle mass after having had 3 shoulder replacement surgeries. A long surgical scar eexisted anteriorly over the deltoid-pectoral junction. The left side was deeper (more tissue deficient) than that of the right, Before proceeding with deltoid implants soft tissue volume restoration over the scar lines was needed.

 As a first stage procedure before implant placement, the areas of graft implantation were marked over the scars.
As a first stage procedure before implant placement, the areas of graft implantation were marked over the scars.

 The anterior shoulder scars were opened and skin flaps raised over the desired implanted area.
The anterior shoulder scars were opened and skin flaps raised over the desired implanted area.

 Large dermal-fat graft swere harvested from the flanks and thin overlying epithelium removed. The dermal-fat grafts were shaped to fit the defect areas.
Large dermal-fat graft swere harvested from the flanks and thin overlying epithelium removed. The dermal-fat grafts were shaped to fit the defect areas.

 The grafts were implanted, dermis side upm sutures into the pocket at all corners and the overlying skin closed
The grafts were implanted, dermis side upm sutures into the pocket at all corners and the overlying skin closed
Discussion
Large dermal-fat grafts can be a useful option for correcting shoulder soft-tissue asymmetries, but they’re not commonly discussed in the same way as facial or breast applications—so the indications and limitations matter a lot.
Conceptually, you’re using a composite graft (dermis + attached fat) to provide:
- Volume (fat component)
- Structural stability and resistance to resorption (dermis component)
That makes them different from standard lipo-fat grafting, especially in areas like the shoulder where:
- Skin is thicker
- Motion is high
- Shear forces can compromise pure fat graft take
When they make sense in the shoulder
Large dermal-fat grafts are most appropriate when the asymmetry is:
- Focal and contour-based (not diffuse volume deficiency)
- Associated with soft tissue deficiency, not just muscle imbalance
- Post-traumatic or post-surgical (e.g., deltoid contour loss, clavicular prominence, AC joint region irregularity)
- Stable defects, not evolving conditions
They can also be useful in:
- Congenital asymmetry (e.g., mild Poland-like presentations without major muscle absence)
- Implant camouflage situations (less common in shoulder vs chest)
Advantages over fat grafting alone
- Lower resorption variability (dermal scaffold helps)
- More predictable shape retention
- Better for defined contour defects rather than generalized volume
- Less dependent on perfect recipient bed vascularity (to a degree)
Limitations / challenges
This is where reality pushes back a bit:
- Size constraints
- “Large” grafts risk central necrosis if they exceed revascularization capacity
- Shoulder region is not as forgiving as face
- Contour visibility
- Shoulder skin is relatively thin over bony landmarks ? graft edges can show if not feathered well
- Mobility
- Deltoid motion ? shear ? risk of partial loss or fibrosis
- Donor site morbidity
- Typically gluteal fold or lower abdomen
- Large grafts = noticeable donor scar
- Fixation
- Requires secure pocketing and sometimes suturing to prevent migration
Technical considerations
- Layered placement rather than one thick block when possible
- Meticulous pocket creation (subfascial vs subcutaneous depending on defect)
- Immobilization post-op (often underappreciated for shoulder cases)
- Consider combining with:
- Fat grafting (hybrid approach) for edge blending
- Local tissue rearrangement if skin deficiency exists
Alternatives (often more practical)
Depending on the defect, these are frequently used instead:
- Autologous fat grafting (serial sessions)
More adaptable for broad asymmetry - Silicone or custom implants
Rare in shoulder, but possible for structural deficits - Muscle flaps (e.g., latissimus, local advancement)
For larger or dynamic defects - Allograft dermal matrices
Occasionally used, but less volumetric than autologous dermal-fat
Bottom line
Dermal-fat grafts can work well for moderate, well-defined shoulder contour defects, especially when you need more structural persistence than what fat injections can achieve.
Dr Barry Eppley
Plastic Surgeon