


 The ogee curve is one of the most important visual concepts in facial aesthetics and has increasing relevance in the design of custom facial implants. In facial analysis, the ogee curve refers to the flowing double-S contour seen on the oblique view of the face that extends from the lateral brow and orbital rim, sweeps outward over the malar eminence, and then curves inward into the submalar and midfacial region. It is not a discrete anatomical structure but rather a compositesoft tissue contour produced by the relationship between the underlying skeleton, fat distribution, skin thickness, and facial projection patterns.
The ogee curve is one of the most important visual concepts in facial aesthetics and has increasing relevance in the design of custom facial implants. In facial analysis, the ogee curve refers to the flowing double-S contour seen on the oblique view of the face that extends from the lateral brow and orbital rim, sweeps outward over the malar eminence, and then curves inward into the submalar and midfacial region. It is not a discrete anatomical structure but rather a compositesoft tissue contour produced by the relationship between the underlying skeleton, fat distribution, skin thickness, and facial projection patterns.
The aesthetic importance of the ogee curve lies in its ability to create facial dimensionality and visual harmony. Faces with a well-defined ogee curve tend to appear youthful, structured, and aesthetically balanced because the transition between the orbit, cheek prominence, and midface is smooth and continuous rather than flat or vertically linear. Aging, skeletal deficiency, trauma, congenital asymmetry, or prior surgery can diminish or distort this contour, producing a flatter or more hollow midface appearance.
 In implant design, the ogee curve becomes particularly useful because it converts a subjective aesthetic observation into a reproducible three-dimensional design principle. Rather than merely augmenting “cheek volume,” the implant must shape the spatial relationship between multiple facial zones. The implant therefore influences not only projection but also contour flow, curvature transition, and the distribution of convexity and concavity across the midface.
In implant design, the ogee curve becomes particularly useful because it converts a subjective aesthetic observation into a reproducible three-dimensional design principle. Rather than merely augmenting “cheek volume,” the implant must shape the spatial relationship between multiple facial zones. The implant therefore influences not only projection but also contour flow, curvature transition, and the distribution of convexity and concavity across the midface.
The upper portion of the ogee curve begins near the lateral orbital rim and temporal-cheek junction. In custom implant design, this region often requires careful tapering and blending to avoid an abrupt fullness adjacent to the lower eyelid or lateral canthus. Excessive fullness in this superior zone creates an unnatural “overfilled” appearance and can feminize a male face unintentionally. Consequently, implant thickness in this region is usually thinner and more feathered.
The central convexity of the ogee curve corresponds to the malar prominence and represents the point of maximum projection. This is typically the dominant design feature in custom cheek implants. Implant thickness, projection vector, and lateral extension are all determined by where the designer wishes the apex of the cheek to appear. In women, this apex is often broader, smoother, and slightly more anterior. In men, the projection is usually higher, sharper, and more laterally positioned along the zygomatic body and arch to create a stronger skeletal appearance.
The inferior concavity of the ogee curve transitions into the submalar and nasolabial region. Failure to preserve this lower inward sweep can create an unnaturally round or “apple cheek” appearance. This is a common limitation of generic implants and filler augmentation where isolated volume addition ignores the overall contour geometry of the face. Custom implants allow deliberate preservation of this inferior concavity through controlled tapering and selective volume distribution.
The ogee curve is best evaluated in the 45-degree oblique view because frontal views compress facial depth and lateral views obscure the double-curvature relationship. For this reason, implant design assessment should always include oblique renderings during virtual surgical planning. Many implant designs that appear satisfactory frontally may look excessively projected or geometrically unnatural once viewed obliquely.
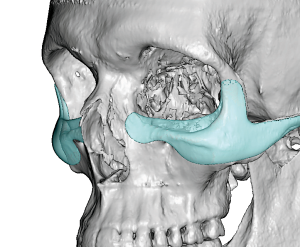
In custom infraorbital-malar implants, the ogee principle becomes even more important because the implant spans multiple anatomical regions simultaneously. The implant must create continuity between the infraorbital rim, anterior cheek, and zygomatic body without abrupt changes in contour. This requires careful management of implant edge transitions, projection gradients, and surface curvature. Modern CAD design software allows manipulation of these parameters with much greater precision than standard stock implants.
The ogee curve also varies according to gender, ethnicity, age, and aesthetic goals. Female ogee curves are usually characterized by softer transitions, broader cheek fullness, and smoother curvature continuity. Male ogee curves generally emphasize skeletal angularity, stronger zygomatic definition, and reduced lower cheek fullness. Ethnic considerations are equally important because midfacial skeletal architecture differs substantially across populations, altering how cheek projection interacts with surrounding facial structures.
From a biomechanical standpoint, the soft tissue envelope strongly influences how the ogee curve manifests externally after implantation. Thick soft tissue may blunt skeletal definition, whereas thin soft tissue can exaggerate implant edges or projection. Thus, implant design cannot rely solely on skeletal augmentation measurements; it must anticipate soft tissue behavior and postoperative draping characteristics.
One of the greatest advantages of custom implants over fillers is the ability to establish a stable skeletal foundation for the ogee contour. Fillers can transiently simulate portions of the curve by adding localized volume, but they often fail to reproduce the structural transitions across the entire midface. Furthermore, fillers tend to create diffuse expansion rather than directional skeletal projection. Custom implants instead reposition the foundational contours from beneath the soft tissue, producing more durable and anatomically coherent changes.
In modern facial implant design, the ogee curve therefore functions as both an aesthetic target and a geometric design strategy. It guides implant thickness distribution, determines projection vectors, influences tapering zones, and helps define how augmented regions integrate with surrounding facial anatomy. Properly designed implants do not merely enlarge the cheek; they restore or create a balanced three-dimensional facial flow that appears natural from all viewing angles.
Dr. Barry Eppley
Plastic Surgeon