

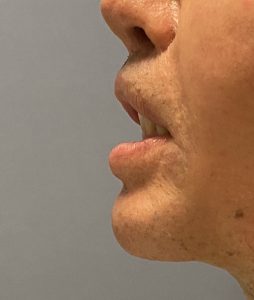

 Lower lip incompetence, often associated with soft tissue chin pad ptosis (sagging), is a difficult problem to satisfactorily correct. It is often associated with loss of chin pad support from implant removal or intraoral chin bone reduction from shaving or a setback sliding genioplasty. As the chin pad loses its attachment to the bone a sag develops which drags the lower lip down with it. At rest the lower lip sag is most evident centrally and the lower lip may even roll out exposed more of the wet mucosa. Forced lip competence can usually be done and this is how the patient often masks the problem in public.
Lower lip incompetence, often associated with soft tissue chin pad ptosis (sagging), is a difficult problem to satisfactorily correct. It is often associated with loss of chin pad support from implant removal or intraoral chin bone reduction from shaving or a setback sliding genioplasty. As the chin pad loses its attachment to the bone a sag develops which drags the lower lip down with it. At rest the lower lip sag is most evident centrally and the lower lip may even roll out exposed more of the wet mucosa. Forced lip competence can usually be done and this is how the patient often masks the problem in public.
Getting the chin pad back up and achieving lip competence is a difficult challenge and numerous strategies have been advocated to do so…with varying degrees of sustained success. I have come to learn that a five level approach to chin pad repositioning, incorporating many of the known methods, needs to be considered in each patient. Not every patient will need all five levels of support and resttachment but some will.
 The first level is that of the bone at the bottom of the chin pad. Adding a supporting ledge whether it be an implant or a sliding genioplasty may need to be done particularly if it does not produce an unaesthetic appearance. (too much chin projection) One can debate which method is better and there are arguments to be made for either an autogenous or alloplastic supporting ledge. This is more patient preference and surgeon comfort with either augmentative procedure.
The first level is that of the bone at the bottom of the chin pad. Adding a supporting ledge whether it be an implant or a sliding genioplasty may need to be done particularly if it does not produce an unaesthetic appearance. (too much chin projection) One can debate which method is better and there are arguments to be made for either an autogenous or alloplastic supporting ledge. This is more patient preference and surgeon comfort with either augmentative procedure.
 The next level is bringing up the lowest of the soft tissue chin with suture fixation to a mid-bone level. This is most easily done with a sliding genioplasty as that is a convenient point for suture attachment to the fixation plate. If no method of chin augmentation is being done then this would be the first level of suture anchor fixation to the bone.
The next level is bringing up the lowest of the soft tissue chin with suture fixation to a mid-bone level. This is most easily done with a sliding genioplasty as that is a convenient point for suture attachment to the fixation plate. If no method of chin augmentation is being done then this would be the first level of suture anchor fixation to the bone.

 The third level is mentalis muscle fixation to the highest bone point which would be at the interdental level. This requires a small suture anchor placed between the roots of the central incisors.
The third level is mentalis muscle fixation to the highest bone point which would be at the interdental level. This requires a small suture anchor placed between the roots of the central incisors.
 The fourth level is whatever soft tissue cuff exists underneath the vestibular mucosa and the higher up muscle fibers of the mentalis muscle. This superior cuff of tissue may not be present in some patients.
The fourth level is whatever soft tissue cuff exists underneath the vestibular mucosa and the higher up muscle fibers of the mentalis muscle. This superior cuff of tissue may not be present in some patients.
 The fifth and last level, and the one most frequently overlooked is shortening the depth of the vestibule. If the chin pad has been sufficiently raised by the prior three or four levels of soft tissue fixation there will be a visible discrepancy between the two sides of the intraoral incision. The outer labial incision level will be much higher than the ‘dental’ side of the incision. Rather than just pulling those two mucosal incisional sides together, the vestibular mucosa below the mucogingival junction should be excised so that the two sides of the incision are level. When this is closed the depth of the vestibule is shortened and the fifth layer of support is completed.
The fifth and last level, and the one most frequently overlooked is shortening the depth of the vestibule. If the chin pad has been sufficiently raised by the prior three or four levels of soft tissue fixation there will be a visible discrepancy between the two sides of the intraoral incision. The outer labial incision level will be much higher than the ‘dental’ side of the incision. Rather than just pulling those two mucosal incisional sides together, the vestibular mucosa below the mucogingival junction should be excised so that the two sides of the incision are level. When this is closed the depth of the vestibule is shortened and the fifth layer of support is completed.
A comprehensive approach to chin pad ptosis and lower lip incompetence requires consideration of different levels of support and suspension. Rarely does ever one level of support work to raise the lower lip and almost always three or more levels are needed for a satisfactory level of improvement.
Dr. Barry Eppley
Indianapolis, Indianapolis