

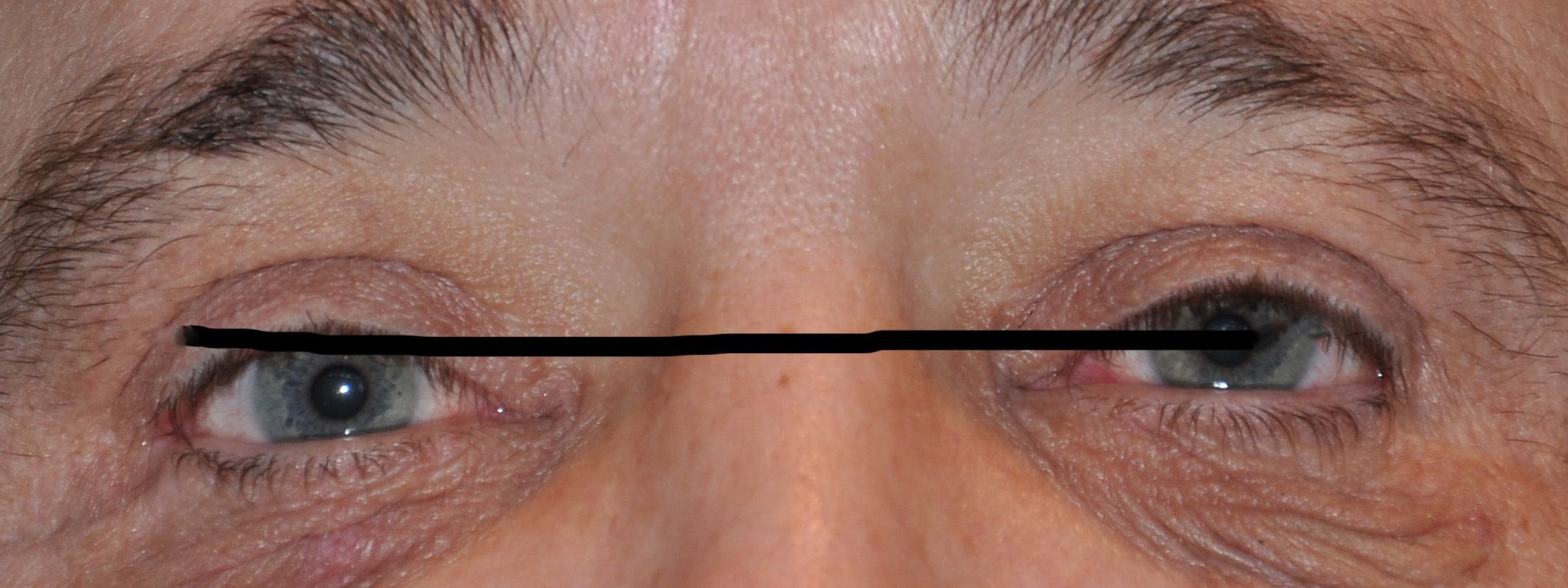
 Vertical orbital dystopia is a frequent feature of many facial asymmetry patients. When facial asymmetry affects the midface region most of the time some form of globe dystopia will be present. It is perceived most easily by the difference in the horizontal level of the pupils.
Vertical orbital dystopia is a frequent feature of many facial asymmetry patients. When facial asymmetry affects the midface region most of the time some form of globe dystopia will be present. It is perceived most easily by the difference in the horizontal level of the pupils.
Orbital dystopia is always most clearly seen in pictures as the eyes look ‘off’. This is where patients will notice it the most as well as when looking directly in the mirror. (or in selfies) There will be one good eye and the affected eye will usually be sitting lower. It is rare that the affected eye is the higher one. For unknown reasons in my experience vertical orbital dystopia occurs much more frequently in the right eye.
The most important step when the eyes appear at different levels is to make the proper diagnosis. This will require a 3D CT scan of the entire face and not just the orbits. Aesthetic (non-craniofacial) orbital dystopia usually has other facial asymmetries as well particularly of the superior brow bone and the inferior cheeks. The entire orbital skeletal box is lower. As a result, the eyebrow and brow bone will also be lower, the upper eyelid may have some mild ptosis and the cheek will be flatter and asymmetric.
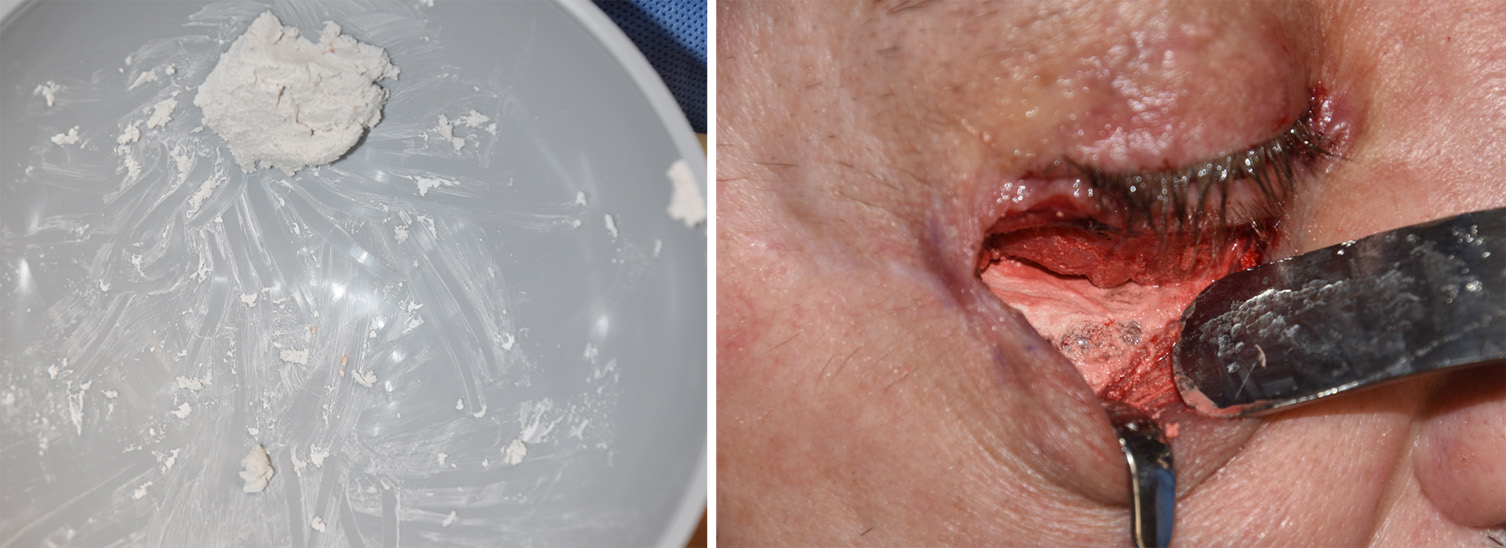 Mild cases (2 to 5mms) of vertical orbital dystopia can be treated by numerous extracranial techniques. Augmentation of the anterior orbital floor (and in some cases the inferior orbital rim), a brow lift and cheek augmentation are the three main skeletal techniques. While numerous implant materials can be used for the orbital bone, including autologous bone grafts, I find the use of hydroxyapatite cement (HA cement) to be very effective. It is easy to apply and shape to the orbital floor and up over the inferior orbital rim if needed.
Mild cases (2 to 5mms) of vertical orbital dystopia can be treated by numerous extracranial techniques. Augmentation of the anterior orbital floor (and in some cases the inferior orbital rim), a brow lift and cheek augmentation are the three main skeletal techniques. While numerous implant materials can be used for the orbital bone, including autologous bone grafts, I find the use of hydroxyapatite cement (HA cement) to be very effective. It is easy to apply and shape to the orbital floor and up over the inferior orbital rim if needed.
 In uncommon cases an adjunctive strategy can be to lower the opposite eye as well. If the affected eye can not be adequately raise due to the amount of horizontal pupillary disccrepancy (4mms or greater) the opposite eye can be slightly lowered. This is done by removing part of the bone on the anterior orbital floor. Short of a full orbital decompression, the goal is to achieve a 1 to 2mm lowering of the globe. This dual approach raises the lower eye and very slightly lowers the opposite eye.
In uncommon cases an adjunctive strategy can be to lower the opposite eye as well. If the affected eye can not be adequately raise due to the amount of horizontal pupillary disccrepancy (4mms or greater) the opposite eye can be slightly lowered. This is done by removing part of the bone on the anterior orbital floor. Short of a full orbital decompression, the goal is to achieve a 1 to 2mm lowering of the globe. This dual approach raises the lower eye and very slightly lowers the opposite eye.
In the correction of vertical orbital dystopia, it is also important to be aware of what may happen to the upper eyelid-globe relationship. In most cases of congenital orbital dystopia the upper eyelid follows the eye to maintain a normal appearing upper eyelid to globe relationship. But as the lower eye is surgically lifted, the eye can be come more buried under the upper eyelid. Ptosis repair may be needed to get the eyelid back up higher on the iris.
Dr. Barry Eppley
Indianapolis, Indiana