


Introduction
The most reliable method of calf augmentation is with the use of implants.. Fat injections may benefit patients who have adequate donor sites and can tolerate their unpredictable volume retention, but most muscle augmentations get the most predictable and effective results from implants. Like most extremity implants, subfascial placement inside the muscle sheath is ideal as it provides a direct augmentation to the muscle. The gliding nature of the muscle inside the fascial sheath needed for flexion and extension movements provides a working space for the placement of an implant. Because of the shape of the gastrocnemius muscles calf implants are longer than they are wider or their length is greater than their width. The incisions used to place calf take advantage of a natural skin crease within the popliteal fossa (behind the knee), taking advantage of a natural skin crease near a movable joint.
Muscle Anatomy and Aesthetic Goals
 The gastrocnemius muscle is composed of two paired muscles:
The gastrocnemius muscle is composed of two paired muscles:
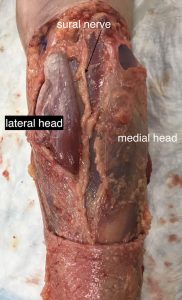
- Medial gastrocnemius: the larger of the two by about a third and is the most visible from the front, it has the most important effect on calf size and shape..
- Lateral gastrocnemius: the smaller of the pair and is not visible from the front with projection primarily toward the back.
While all calf augmentation patients for aesthetic purposes need medial or inner muscle implants, total calf augmentation is both medial and lateral implants. Men more commonly get two implants per leg as they often seek a larger and more defined lower leg appearance. Women however often only want medial muscle implants as their goal is a lower leg contour improvement.
Incisions
 The incisions used to place calf take advantage of a natural skin crease within the popliteal fossa (behind the knee). This takes advantage of a natural skin crease near a movable joint. A single incision is used for each muscle belly which provides direct linear access to the muscle below it. It is important to recognize that the fascia seen right below the incision is not that of the gastrocnemius muscle but that of the hamstring muscles. Further down from that fascia lies that of the gastrocnemius muscle.
The incisions used to place calf take advantage of a natural skin crease within the popliteal fossa (behind the knee). This takes advantage of a natural skin crease near a movable joint. A single incision is used for each muscle belly which provides direct linear access to the muscle below it. It is important to recognize that the fascia seen right below the incision is not that of the gastrocnemius muscle but that of the hamstring muscles. Further down from that fascia lies that of the gastrocnemius muscle.
While a convenient location for the incision the extension of the knee makes great scar results challenging due to that movement tension.
Key Nerve Considerations
Proper placement requires awareness of the surrounding nerve anatomy:
- Sural nerve:
 A sensory nerve running between the gastrocnemius heads, supplying sensation to the back of the leg, outer ankle, and lateral foot. It lies outside the fascial covering of both muscles. As long as dissection remains within the muscle fascia and does not cross the midline, the risk of sural nerve is low. This is why two separate incisions are used to avoid crossing the midline between the twi muscles.
A sensory nerve running between the gastrocnemius heads, supplying sensation to the back of the leg, outer ankle, and lateral foot. It lies outside the fascial covering of both muscles. As long as dissection remains within the muscle fascia and does not cross the midline, the risk of sural nerve is low. This is why two separate incisions are used to avoid crossing the midline between the twi muscles. - Common peroneal nerve:
A mixed motor and sensory nerve responsible for foot dorsiflexion and eversion. It travels through the popliteal fossa and around the posterior fibular neck. Its course can be very close to the incision for a lateral calf implant. Careful blunt dissection is essential to identify and preserve it. If encountered, the implant should be passed medial to the nerve, with gentle retraction to avoid a stretch injury to the nerve and the risk of a postoperative foot drop.
 A sensory nerve running between the gastrocnemius heads, supplying sensation to the back of the leg, outer ankle, and lateral foot. It lies outside the fascial covering of both muscles. As long as dissection remains within the muscle fascia and does not cross the midline, the risk of sural nerve is low. This is why two separate incisions are used to avoid crossing the midline between the twi muscles.
A sensory nerve running between the gastrocnemius heads, supplying sensation to the back of the leg, outer ankle, and lateral foot. It lies outside the fascial covering of both muscles. As long as dissection remains within the muscle fascia and does not cross the midline, the risk of sural nerve is low. This is why two separate incisions are used to avoid crossing the midline between the twi muscles. A mixed motor and sensory nerve responsible for foot dorsiflexion and eversion. It travels through the popliteal fossa and around the posterior fibular neck. Its course can be very close to the incision for a lateral calf implant. Careful blunt dissection is essential to identify and preserve it. If encountered, the implant should be passed medial to the nerve, with gentle retraction to avoid a stretch injury to the nerve and the risk of a postoperative foot drop.
A mixed motor and sensory nerve responsible for foot dorsiflexion and eversion. It travels through the popliteal fossa and around the posterior fibular neck. Its course can be very close to the incision for a lateral calf implant. Careful blunt dissection is essential to identify and preserve it. If encountered, the implant should be passed medial to the nerve, with gentle retraction to avoid a stretch injury to the nerve and the risk of a postoperative foot drop.Subfascial Placement
As noted previously identifying the correct muscle fascia is the first important step. Like a stair step from the incision the gastrocnemius fascia is further south. Make an incision the fascia and look at the orientation of the muscle fibers. If they are clearly running north-south then this is the correct muscle.
In developing the pocket and placing the implant there are differences between the two sides. For medial implants, maximize aesthetic impact by placing them as medially as possible right up against the tibial bone. For lateral implants, keep them completely posterior to avoid injury to the peroneal nerve.
It is important to ensure that the implant pocket dissection is adequate (low enough) so that it does not ride up near the incision. This can be checked after placement by bending the leg at 90 degrees flexion and checking implant position.
Implant Sizes
 Due to the differences in the size of the gastrocnemius muscles smaller implant lengths and widths are need for the lateral muscle. Preoperative sizing is done by measurements of the muscle lengths and widths with the patient standing on their toes. The length of the implant should be a few cms shorter than the external measurements to keep the top part of the implant at a level lower than that of the incision.
Due to the differences in the size of the gastrocnemius muscles smaller implant lengths and widths are need for the lateral muscle. Preoperative sizing is done by measurements of the muscle lengths and widths with the patient standing on their toes. The length of the implant should be a few cms shorter than the external measurements to keep the top part of the implant at a level lower than that of the incision.
Recovery



 Calf implant surgery will cause a fair amount of lower leg and ankle swelling due to their dependent position. The lower leg can look very much like sausages the first week after the surgery particularly if it is combined with other body procedures. This will take several weeks for much of the swelling to dissipate.
Calf implant surgery will cause a fair amount of lower leg and ankle swelling due to their dependent position. The lower leg can look very much like sausages the first week after the surgery particularly if it is combined with other body procedures. This will take several weeks for much of the swelling to dissipate.
Because it is muscle surgery postoperative discomfort is common and walking may initially be uncomfortable. But within a few days it is beneficial to begin lower leg (calf muscle) stretches. This is best done by doing calf flexion on stairs, toes on the step and dropping the heel off the edge, letting the weight of one’s body to stretch the muscle out.
Summary
Calf implants provide effective improvement in lower leg augmentation, but success depends on meticulous attention to anatomy, particularly nerve pathways, and subfascial placement. Due to differences in the medial and lateral gastrocnemius muscles, implant size and pocket placement are different.
Dr. Barry Eppley
World-Renowned Plastic Surgeon