

Calf implants are used for a variety of reasons from aesthetic muscular augmentation to correction of congenital lower leg deformities. (e.g., club foot) They are placed on top of the existing gastrocnemius muscles to provide an external contour change that results in an enhanced lower leg size appearance. Since there are two muscle bellies to the gastrocnemius muscle (medial and lateral heads), it is common to place two implants per leg for maximal lower leg enhancement/reconstruction.
Calf implants are placed from small incisions behind the knee in the popliteal skin crease. This provides access to the fascial lining at the top of the muscle. The standard approach is one incision for each muscle belly/implant. As such when two implants are needed per leg this requires two separate incisions on the back side of the knee.
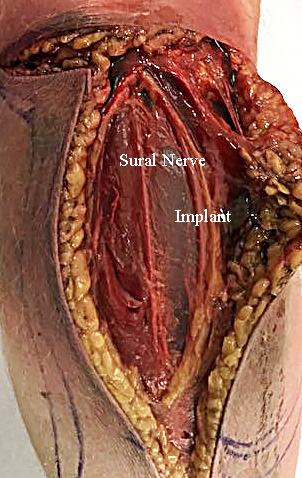 A question one may understandably ask about the incisions for two calf implants is what can’t there just be one incision to place both implants? A look at the anatomy of the calf region will answer that question. The medial and lateral head of the gastrocnemius muscles are separated by an intermuscular septum. Within that septum runs the sural nerve. The sural nerve is a sensory nerve that is composed of branches of the tibial and common fibular nerve that runs down the middle of the calf all the way down to the ankle. It is supples feeling to the side of the foot.
A question one may understandably ask about the incisions for two calf implants is what can’t there just be one incision to place both implants? A look at the anatomy of the calf region will answer that question. The medial and lateral head of the gastrocnemius muscles are separated by an intermuscular septum. Within that septum runs the sural nerve. The sural nerve is a sensory nerve that is composed of branches of the tibial and common fibular nerve that runs down the middle of the calf all the way down to the ankle. It is supples feeling to the side of the foot.
Injury to the sural nerve can cause foot numbness as well as can be a source of chronic pain. Trying to place calf implants from a middle skin incision, placed between the two heads of the muscle, runs the risk of potentially injuring this nerve. In addition it becomes harder to do a proper dissection on either medial or lateral implant pocket without violating the intermuscular septum and creating a ‘unipocket’ where both implants are not separated but touch each other.
Dr. Barry Eppley
Indianapolis, Indiana