

Calf augmentation can be done by two surgical methods. The most historic and reliable is the use of synthetic calf implants. A more recent but far more unpredictable technique is that of fat injections. Each calf augmentation method has its advantages and disadvantages but, like breast augmentation, fat injections are a good volume addition technique in only a very few carefully selected patients.
While calf implants are well known, the surgical method to place them is done by very few plastic surgeons. With good surgical technique, calf augmentation can be done with a good aesthetic outcome and very successful long-term results.
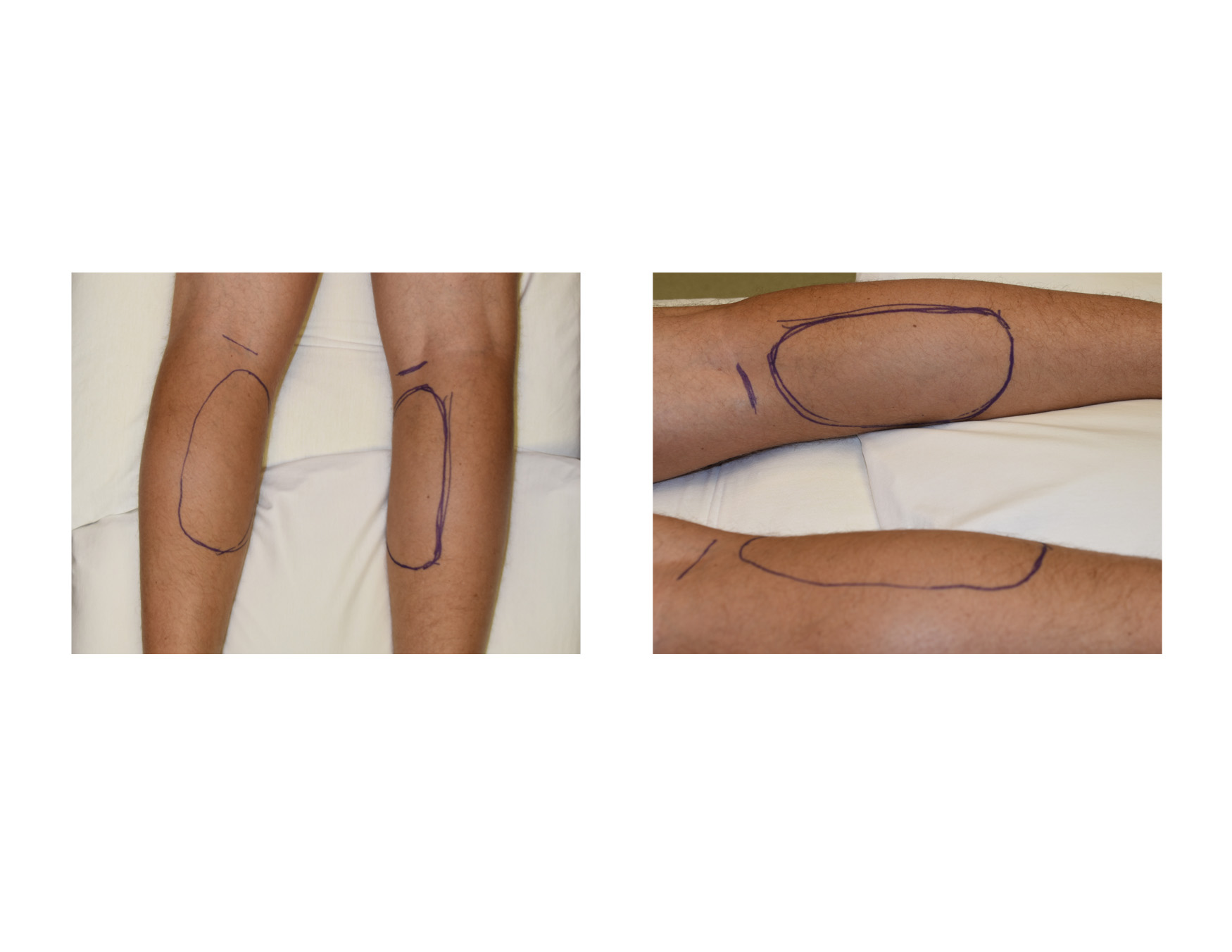 The placement of calf implants is done from incisions behind the knees. A separate incision is need for either medial or lateral implants placed over the gastrocnemius muscles. Each incision does not need to be longer than about 3.5 cms. It should be placed directed in the visible skin crease in the popliteal fossa which is seen even in young patients.
The placement of calf implants is done from incisions behind the knees. A separate incision is need for either medial or lateral implants placed over the gastrocnemius muscles. Each incision does not need to be longer than about 3.5 cms. It should be placed directed in the visible skin crease in the popliteal fossa which is seen even in young patients.
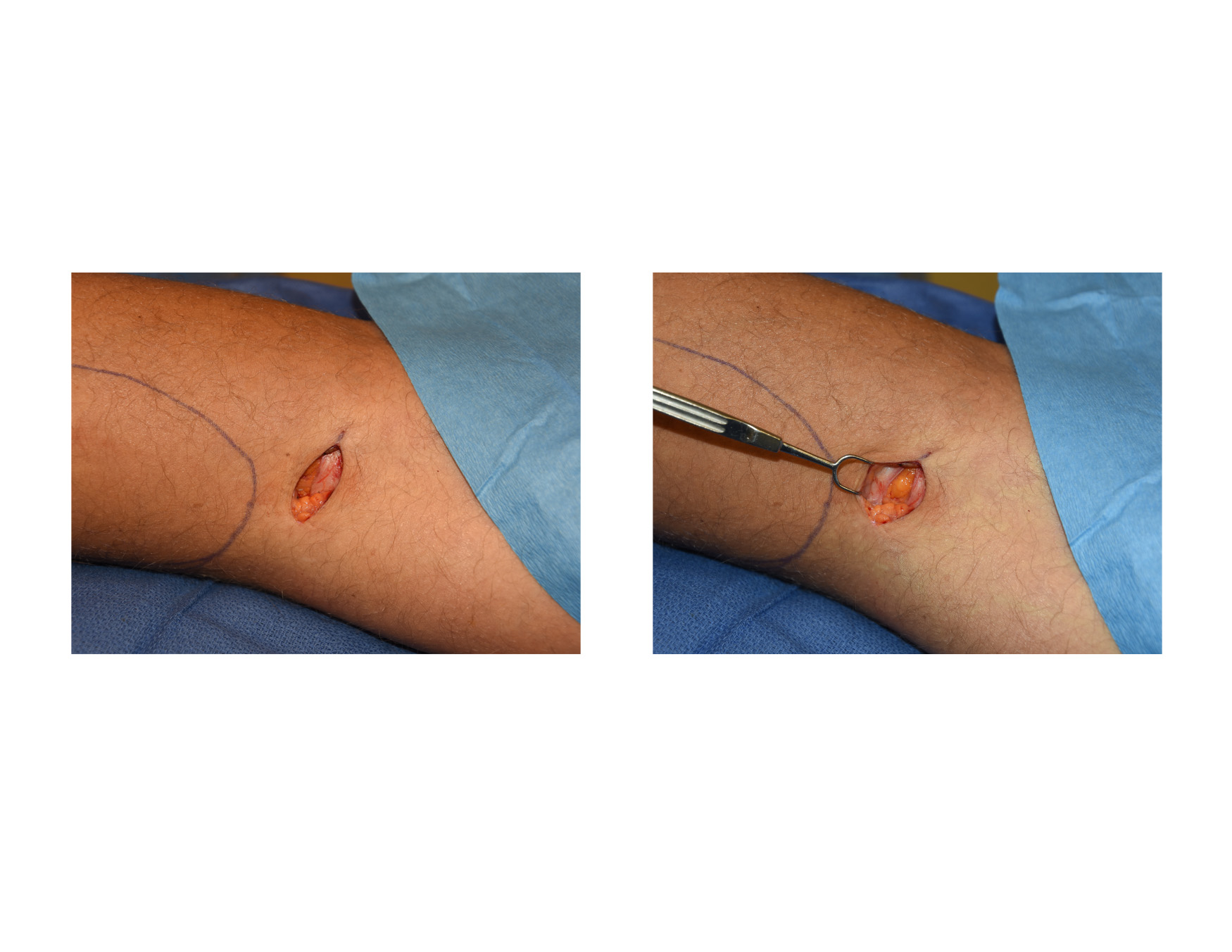 Once the skin incision is made, dissection is carried down through the subcutaneous fat to the the dense fascia layer over the muscle. One may encounter cutaneous sensory nerve branches at the end of the incisions and they should be preserved and pushed aside. Once the fascia is encountered it is incised at the same horizontal length as the skin incision.
Once the skin incision is made, dissection is carried down through the subcutaneous fat to the the dense fascia layer over the muscle. One may encounter cutaneous sensory nerve branches at the end of the incisions and they should be preserved and pushed aside. Once the fascia is encountered it is incised at the same horizontal length as the skin incision.
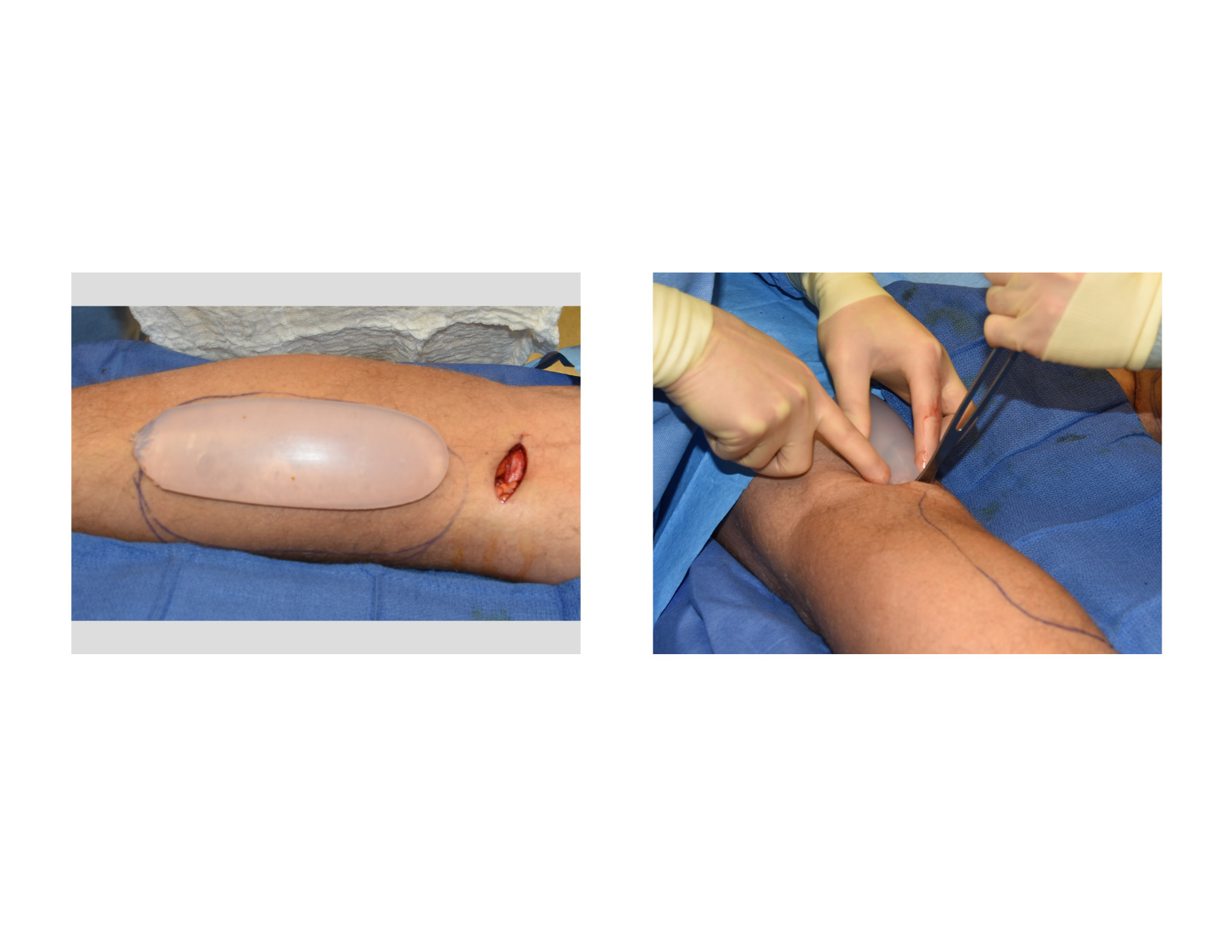
 A subfascial pocket is developed with special instruments that can create the dimensions needed without tearing the overlying fascial lining. It is important the the pocket not be developed too long so that the fascia is not violated at the bottom of the pocket where it gets adherent to the soleus region. Also the pocket should not be developed across the midline union of the gastrocnemius muscles to prevent implant drift. The calf implants are inserted by squeezing them through the skin and fascial incisions. The special double layer design of the calf implants (Implantech body contouring implants) allows them to be compressed and pushed through small incisions without tearing of his soft gel shape.
A subfascial pocket is developed with special instruments that can create the dimensions needed without tearing the overlying fascial lining. It is important the the pocket not be developed too long so that the fascia is not violated at the bottom of the pocket where it gets adherent to the soleus region. Also the pocket should not be developed across the midline union of the gastrocnemius muscles to prevent implant drift. The calf implants are inserted by squeezing them through the skin and fascial incisions. The special double layer design of the calf implants (Implantech body contouring implants) allows them to be compressed and pushed through small incisions without tearing of his soft gel shape.
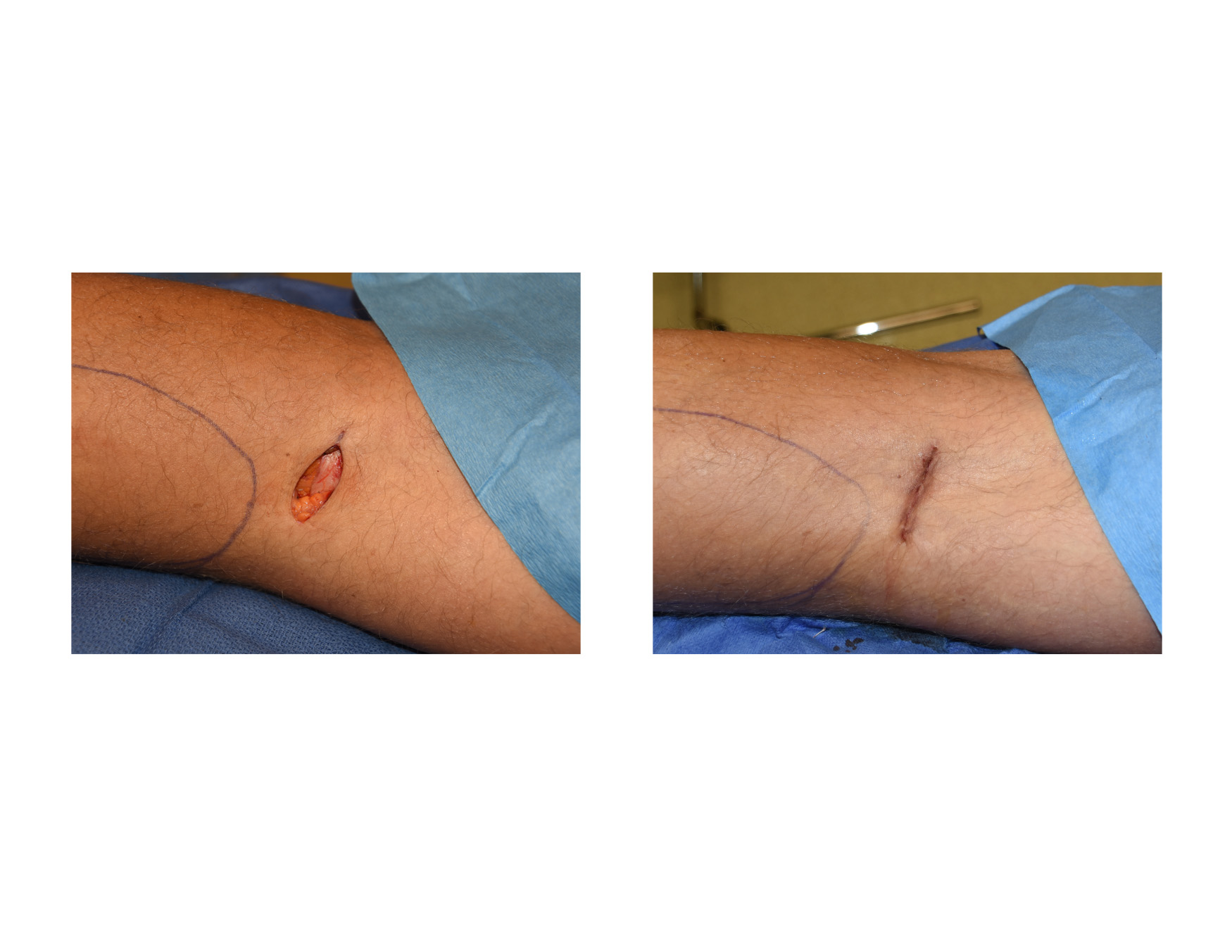 Once positioned into the pocket, the implant should like well below the fascial incision line. In closing the incision, the underlying fascia should not be attempted to be closed. (which often is impossible anyway) Closing the gastrocnemius fascia makes the calf area very tight and increases after surgery pain. A flap of fat should be used to cover the fascial opening. The skin is then closed in two layers with dissolvable sutures. The incision is covered by tapes and the calfs ace wrapped.
Once positioned into the pocket, the implant should like well below the fascial incision line. In closing the incision, the underlying fascia should not be attempted to be closed. (which often is impossible anyway) Closing the gastrocnemius fascia makes the calf area very tight and increases after surgery pain. A flap of fat should be used to cover the fascial opening. The skin is then closed in two layers with dissolvable sutures. The incision is covered by tapes and the calfs ace wrapped.
While calf implants are more invasive and involve a longer recovery than fat injections, well placed subfascial implants provide a permanent method of calf augmentation. The subfascial placement of the implants will require several weeks of recovery until one can resume full physical activities.
Dr. Barry Eppley
Indianapolis, Indiana