

Facial asymmetry is generally the norm, not the exception. The same may be said to be true for any paired body part. Few people have identical facial halfs but most such asymmetries are minor and essentially undetectable. With the asymmetry becomes more than minor (greater than five millimeters or more), however, it may become apparent to more than just the casual eye.
One of the most common reasons for facial asymmetry is the mandible or lower jaw. In my experience, I consider it the most likely facial bone to develop differences between the two sides during growth. This most likely is because of its hinged or joint attachments (TMJ) to the skull where jaw growth is highly influenced by condylar development. Any injury, even minor, to the condyle during growth can cause bone developments differences between the two sides.
When the lower jaw is not symmetrically developed, it can be quite apparent with obvious facial asymmetry and a potential malocclusion. (poor bite) More frequently, however, the face and jaw may be asymmetric but one’s occlusion has good interdigitation. There are many known causes of mandibular asymmetry including a superior altered cranial base (craniosynostosis, torticollis, deformational plagiocephaly), condylar deformities (fractures, hyperplasia, hemifacial microsomia, arthritic degeneration) and external compressive deformation from overlying tumors causing a mass effect.
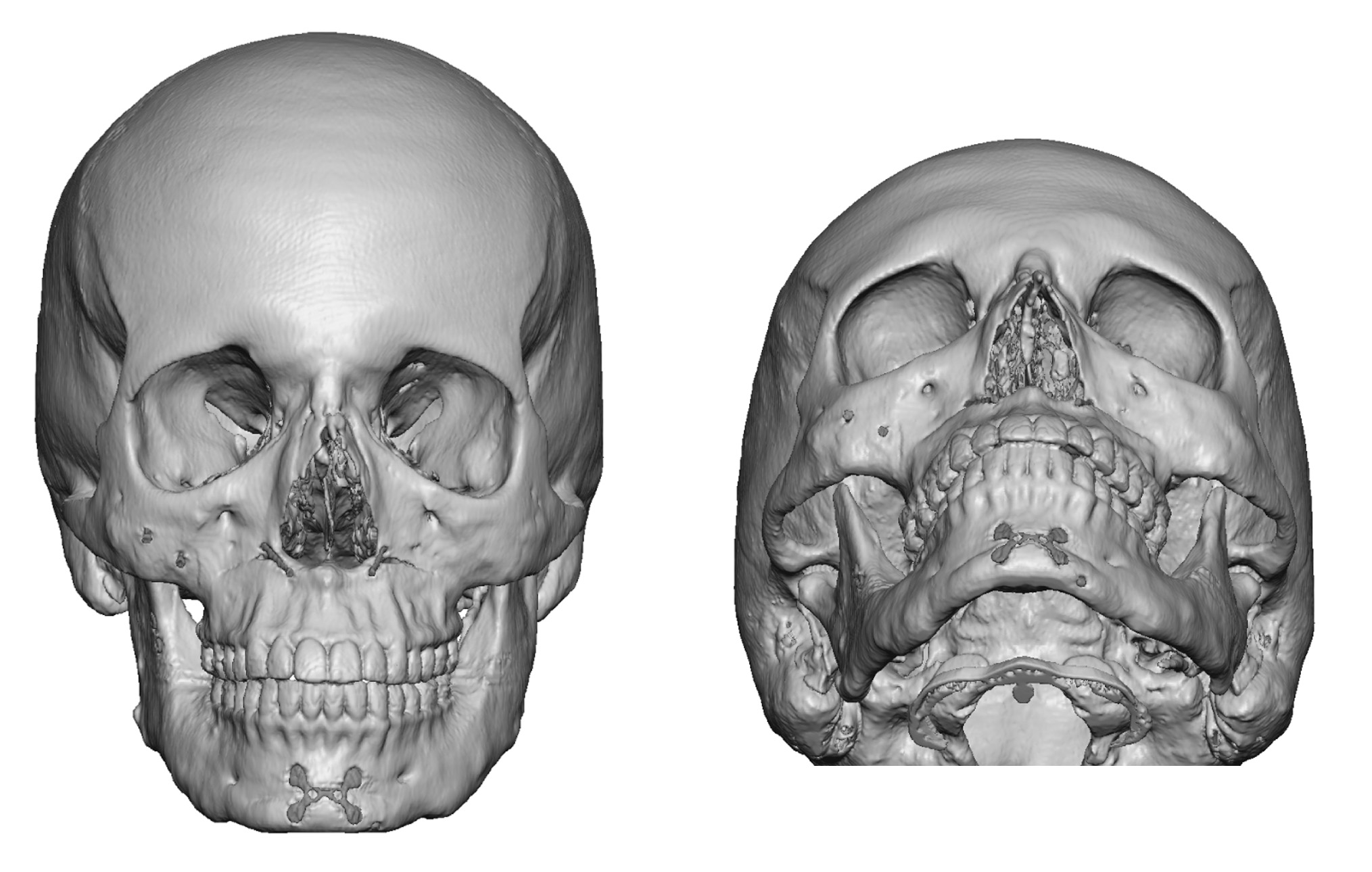 Most commonly, however, I see mandibular-based facial asymmetries in adults which do not have a clearly identifiable cause. Regardless of the reason, known or unknown, the diagnosis only matters from the standpoint of understanding where and how the mandible is asymmetric. A 3-D CT scans is the gold standard by which such jaw asymmetries need to be evaluated. An old style panorex film is helpful, and will clearly show the asymmetry, but its correction requires a 3D implant design approach run most cases. . It allows for tracing and precise measurements of the vertical height of the ramus, the differences in the inferior border of the mandible from side to side, and the symmetry of the two chin halfs.
Most commonly, however, I see mandibular-based facial asymmetries in adults which do not have a clearly identifiable cause. Regardless of the reason, known or unknown, the diagnosis only matters from the standpoint of understanding where and how the mandible is asymmetric. A 3-D CT scans is the gold standard by which such jaw asymmetries need to be evaluated. An old style panorex film is helpful, and will clearly show the asymmetry, but its correction requires a 3D implant design approach run most cases. . It allows for tracing and precise measurements of the vertical height of the ramus, the differences in the inferior border of the mandible from side to side, and the symmetry of the two chin halfs.
When mandibular asymmetry exists with a bite discrepancy or significant cant to the face, strong consideration should be given to a combined treatment plan of orthodontics and corrective maxillary and mandibular osteotomies. This will produce by far the best long-term solution. However, for those patients that do not want or are not capable of going through this program or for more minor asymmetries, a camouflage treatment can be done.
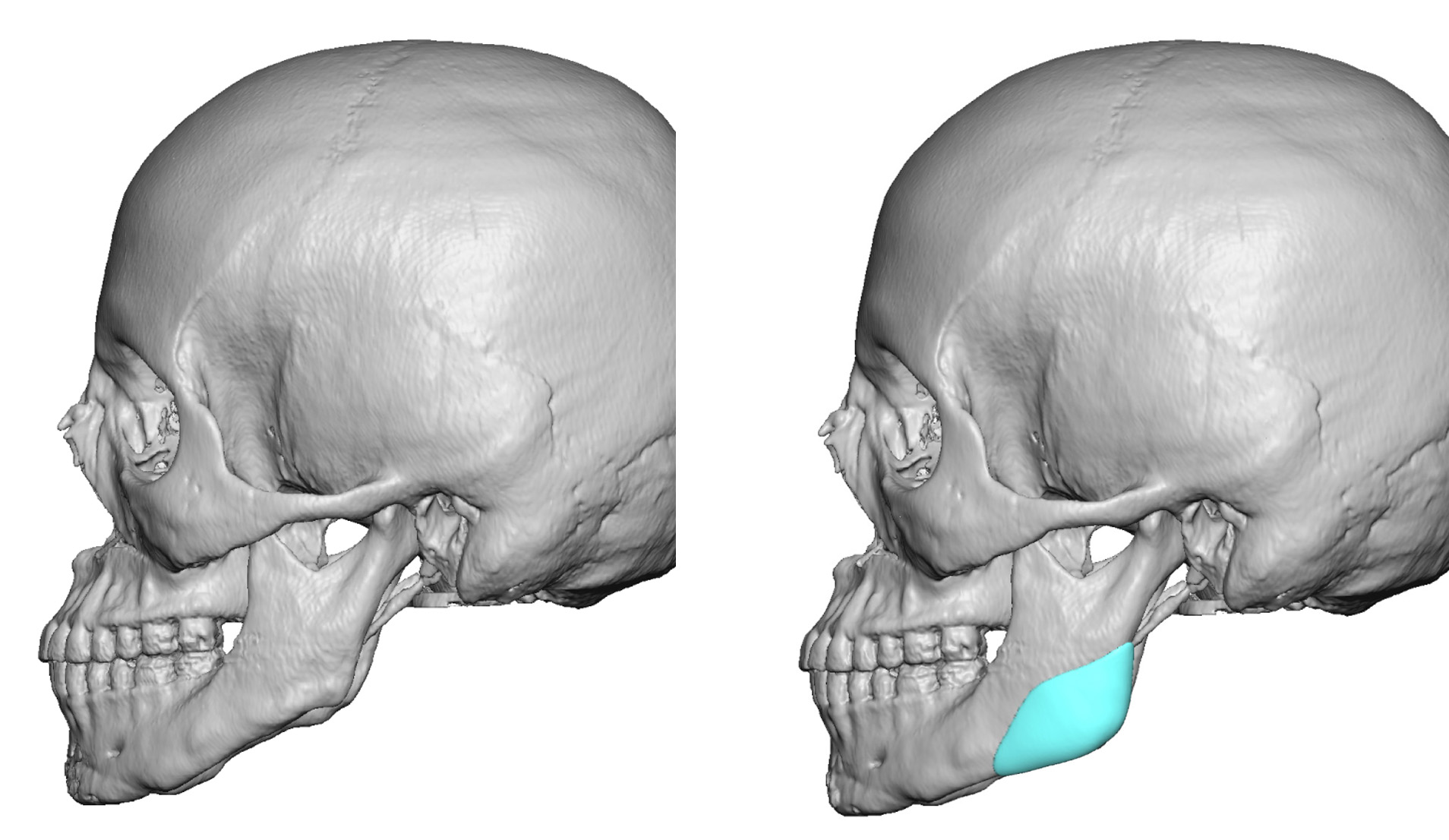 Camouflage treatments for any form of facial asymmetry is largely based on using bone implants for augmentation or removing bone for reduction. For the short posterior (back part) of the mandible, the use of jaw angle implants can be very useful to made it wider and/or longer. Those jaw angle implants which extend or wrap around the lower border are particularly useful as well as more stable. Usually a custom jaw angle implant design approach is best. When the ramus is too long, jaw angle and inferior border ostectomies (bone removal) can be done to better match the other side. Both approaches are done intraorally.
Camouflage treatments for any form of facial asymmetry is largely based on using bone implants for augmentation or removing bone for reduction. For the short posterior (back part) of the mandible, the use of jaw angle implants can be very useful to made it wider and/or longer. Those jaw angle implants which extend or wrap around the lower border are particularly useful as well as more stable. Usually a custom jaw angle implant design approach is best. When the ramus is too long, jaw angle and inferior border ostectomies (bone removal) can be done to better match the other side. Both approaches are done intraorally.
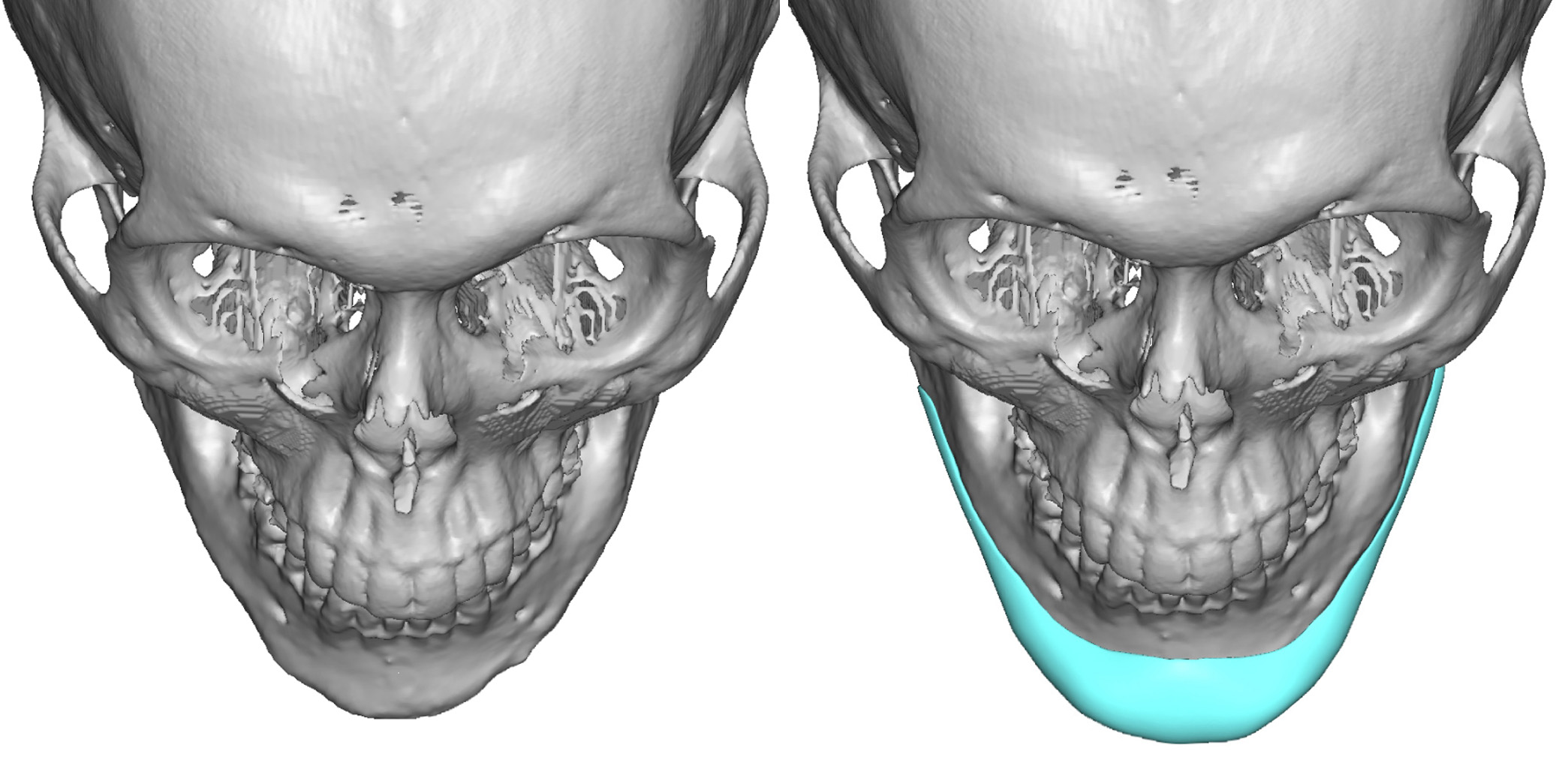 When the asymmetry involves the chin standard chin implants are not usually the best option. If the asymmetry requires augmentation a custom chin implant designs is always the best implant approach. Conversely if reduction for chin asymmetry is needed, cutting and leveling the chin bone can be done.
When the asymmetry involves the chin standard chin implants are not usually the best option. If the asymmetry requires augmentation a custom chin implant designs is always the best implant approach. Conversely if reduction for chin asymmetry is needed, cutting and leveling the chin bone can be done.
Significant correction of mandible-based facial asymmetries can be done by a combination of jaw angle and chin manipulations. Choosing the best options can be done through a good facial analysis and patient discussion as well as a 3D CT scan assessment.
Dr. Barry Eppley
Indianapolis