

Background: The correction of congenital skull deformities with early cranial vault reconstruction is a well established surgical therapy. Such early skull manipulations are based on two fundamental principles of the infant’s skull. First, the bone is thin and can fairly easily be removed, reshaped and re-inserted. Secondly, the osteogenic regenerative power of the dura at such early ages allows any bone defects around the bone reconstruction to fill in with new bone.
But despite the potential osteogenic capability of the dura in infants, full-thickness bone defects still do occur. Often they are small and are at the junction of reassembled skull bone pieces from the initial reconstruction. But in rare cases the skull defects may be much bigger, reflective of bone defects left behind from large bony advancements from contour expansions.
The reconstruction of skull defects in children can be done by a variety of methods. While bone may be considered an ideal material, the successful splitting of cranial bone in children is not an assured outcome. A variety of synthetic materials and implants are available to ‘patch’ such skull defects. Each has their own unique handling characteristics.
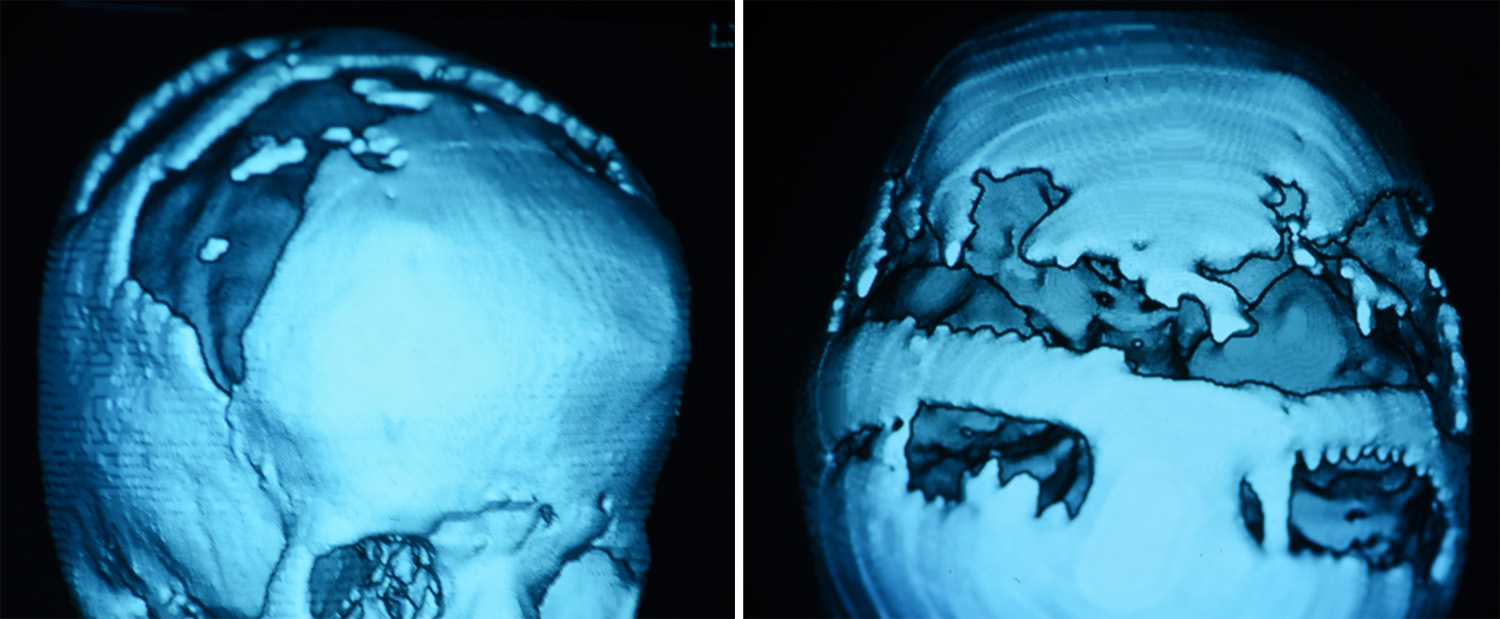 Case Study: This 9 year-old female was originally born with bilateral coronal craniosynostosis for which she underwent a fronto-orbital advancement at 11 months of age. At five years of age it could be seen that large full-thickness defects remained that never filled in with bone from the wake of the fronto-orbital advancements.
Case Study: This 9 year-old female was originally born with bilateral coronal craniosynostosis for which she underwent a fronto-orbital advancement at 11 months of age. At five years of age it could be seen that large full-thickness defects remained that never filled in with bone from the wake of the fronto-orbital advancements.
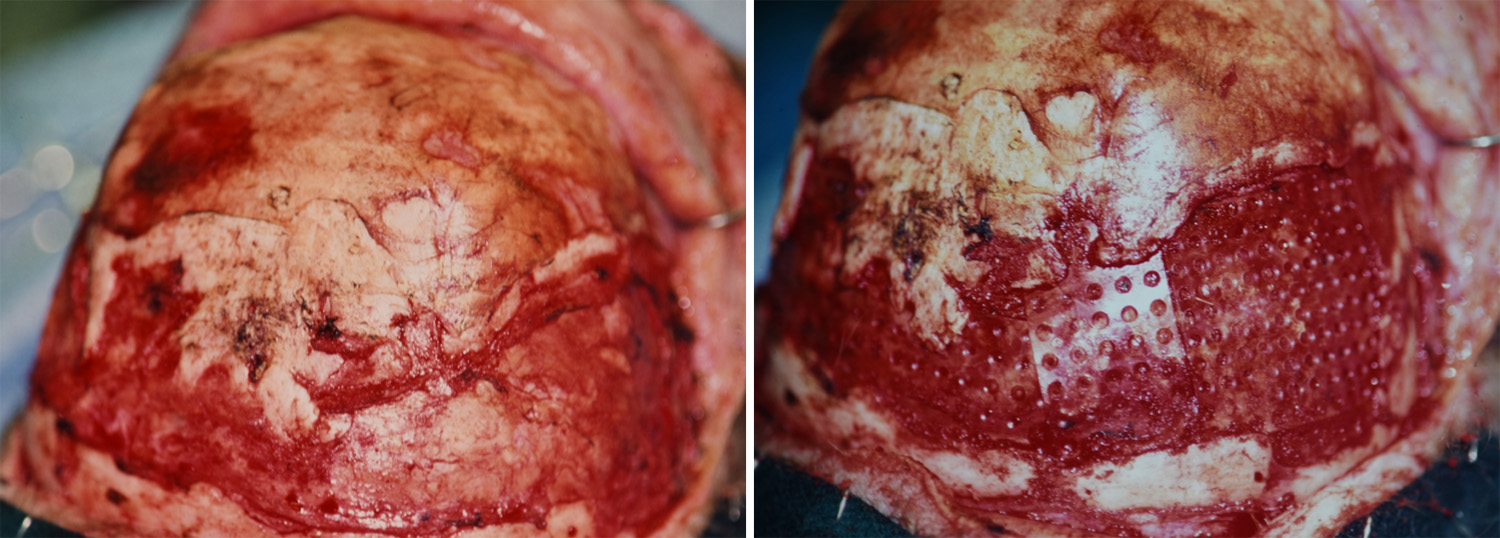
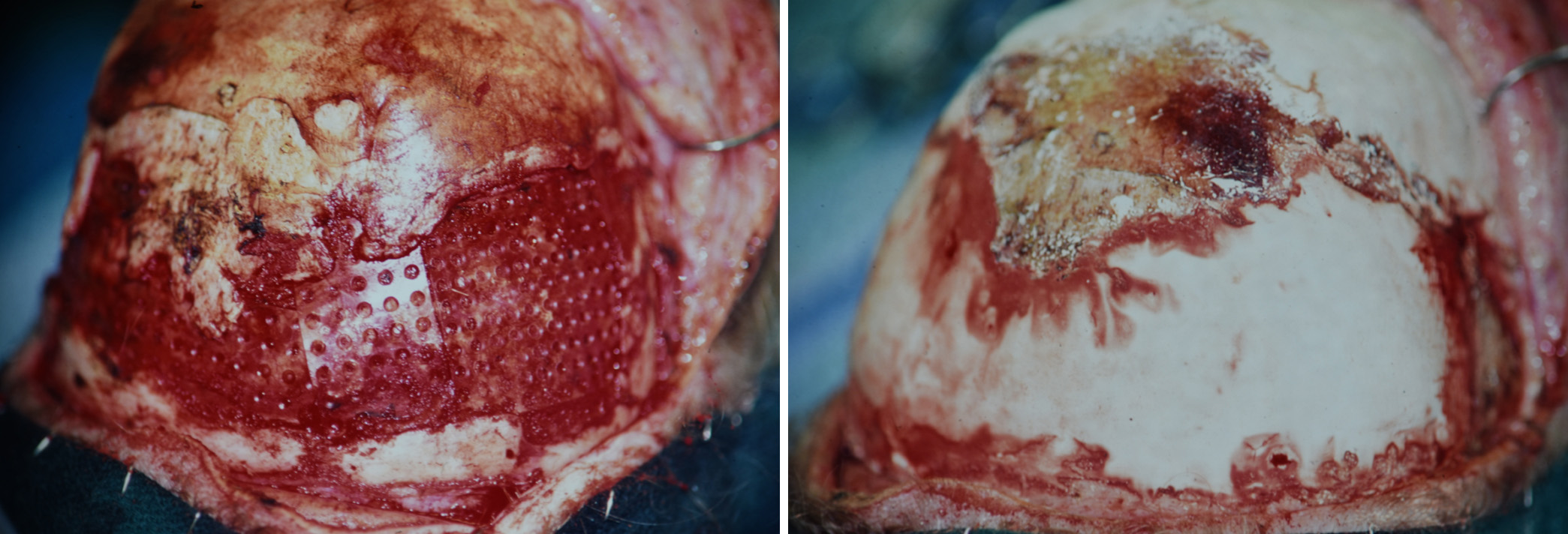
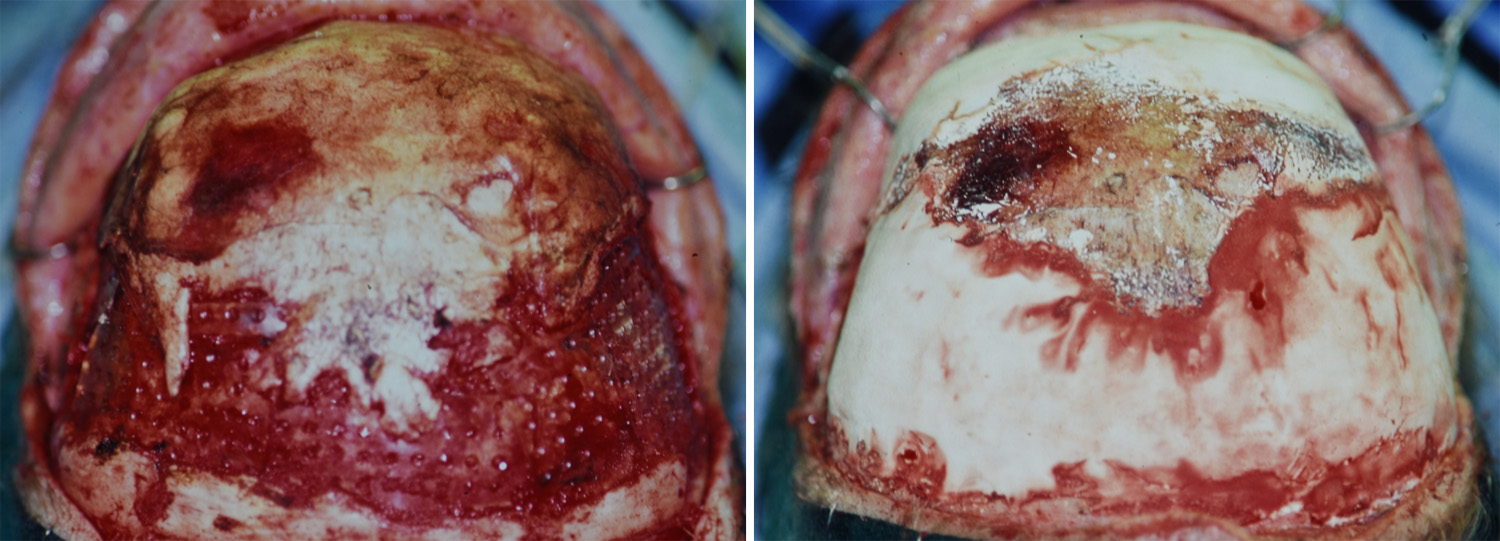
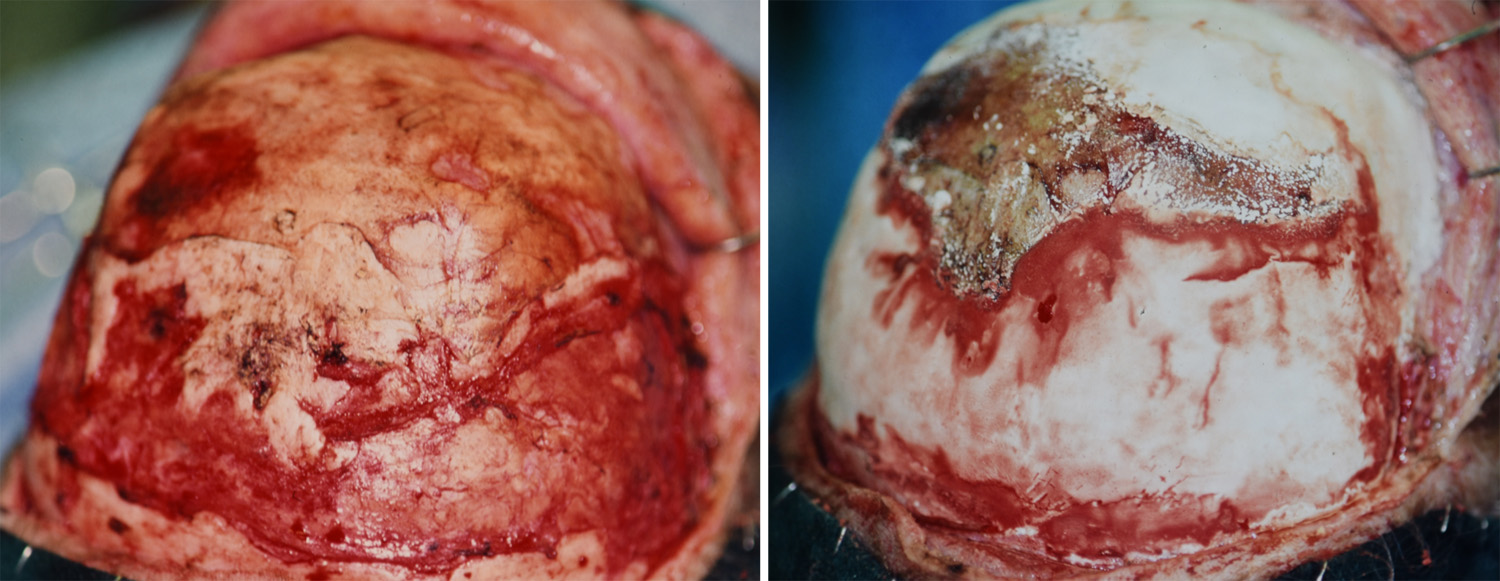 Under general anesthesia, the skull and bone defects were exposed through her original coronal scalp incision. The bone defects were lined with resorbable mesh plates by separating the dura from the bony edges so the plates could be slide under and be held into place. Hydroxyapatite cement was applied onto the plates and built up to the surrounding bone edges for a smooth skull contour.
Under general anesthesia, the skull and bone defects were exposed through her original coronal scalp incision. The bone defects were lined with resorbable mesh plates by separating the dura from the bony edges so the plates could be slide under and be held into place. Hydroxyapatite cement was applied onto the plates and built up to the surrounding bone edges for a smooth skull contour.
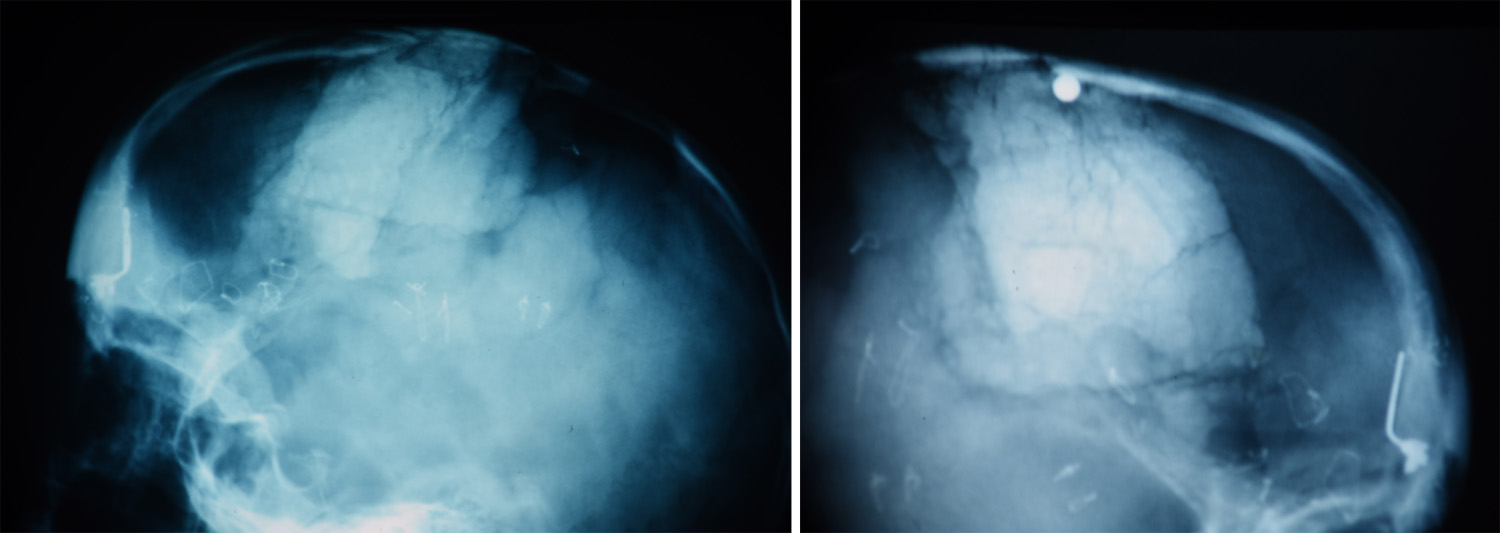 After surgery x-rays show the hydroxyapatite cement, which while containing the inorganic mineral hydroxyapatite, is actually more dense than bone even if it is structurally weaker. The long-term of such hydroxyapatite cements is not resorption and replacement with bone. Rather it will serve as as substrate onto which bone will grow across its outer surface, re-establishing a bony bridge across the defects.
After surgery x-rays show the hydroxyapatite cement, which while containing the inorganic mineral hydroxyapatite, is actually more dense than bone even if it is structurally weaker. The long-term of such hydroxyapatite cements is not resorption and replacement with bone. Rather it will serve as as substrate onto which bone will grow across its outer surface, re-establishing a bony bridge across the defects.
Highlights:
- Full thickness skull defects are not rare after infantile cranial vault reconstruction surgery.
- While hydroxyapatite cement may be the best reconstructive material choice for the pediatric skull, its weak biomechanical properties are not favorable to be used alone.
- Creating a stable floor with resorbable mesh plates allows hydroxyapatite cement to be successfully applied in full thickness skull defects in children.
Dr. Barry Eppley
Indianapolis, Indiana