

Background: The skull is usually depicted as having an oblong shape with an overall smooth surface. While this is usually true, it is prone to have numerous bony irregularities. Most of skull irregularities occur along its suture lines particlerly where the differ suture lines merge. This would be understandable as these are areas of bone union and growth during the development and growth of the skull.
 Although the back of the head is often referred as the occipit (back and lower part of the skull), this does not define the true occipital bone. The occipital bone is located on the lower half of the occiput most of which is not seen externally due to its inward curve down to the base of the skull around the foramen magnum and its coverage by the thick neck muscles. Only the upper portion of the occipital bone is visualized on the back of the head where it merges with the parietal bone through its union by the lambdoidal suture. This is an area that also has a numerous horizontal tissue attachments which creates a series of nuchal lines or ridges.
Although the back of the head is often referred as the occipit (back and lower part of the skull), this does not define the true occipital bone. The occipital bone is located on the lower half of the occiput most of which is not seen externally due to its inward curve down to the base of the skull around the foramen magnum and its coverage by the thick neck muscles. Only the upper portion of the occipital bone is visualized on the back of the head where it merges with the parietal bone through its union by the lambdoidal suture. This is an area that also has a numerous horizontal tissue attachments which creates a series of nuchal lines or ridges.
There are numerous horizontal nuchal lines on the upper occipital region of the skull. The upper nuchal line, the most faint, often called the Mempin line is where the epicranial aponeurosis attaches. The most prominent is the superior nuchal line below it where numerous neck muscles attach including the splenius capitis, trapezius, occipitalis and the sternocleidomastoid.
Because of the lambdoidal suture and the attachments of the neck muscles, it is very prone to irregularities and protrusions across the back of the head. These often appear externally as a raised horizontal ridge that has an irregular shape and feel to it. The shorter one’s hair is the more such bony prominences may appear.
Case Study: This young man was bothered by a raised protrusion on the back of his head. It was a horizontal palpable line of bone that was quite irregular. He had a prior skull surgery that was a brow bone reduction done through a full coronal scalp incision.
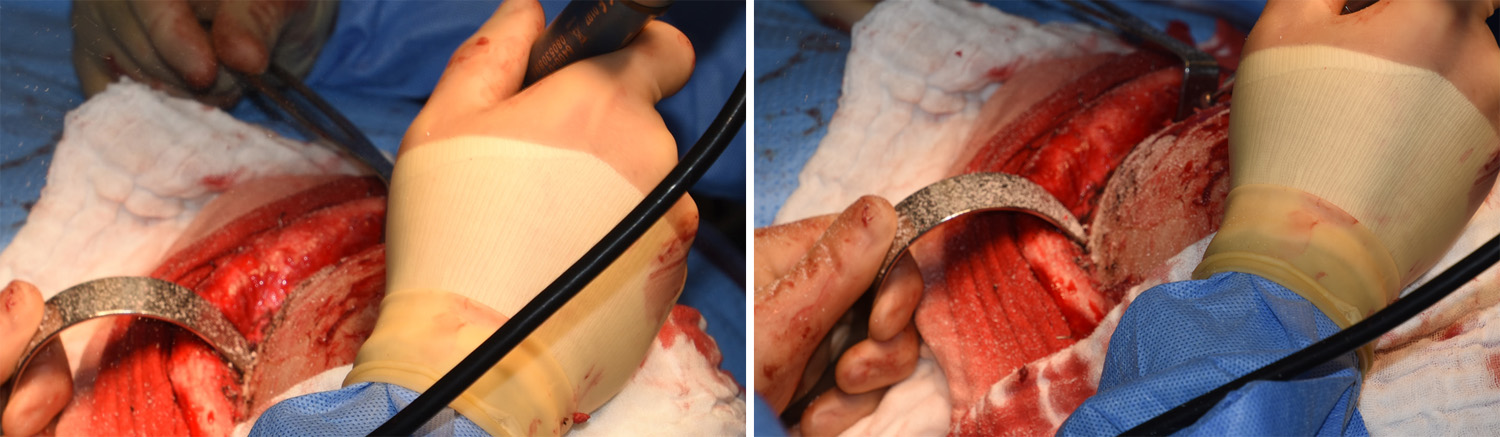 Under general anesthesia and in the prone position his existing coronal scalp incision was used for wide open access to the back of his head. The prominent and irregular ridge of bone along the nuchal ridge was easily identified and reduced by a high-speed handpiece and rotary burr. At the same time the parietal bone above it was reduced as well as the parietal eminences at the sides. Such burin reduction of the skull creates a large amount of bone dust during its execution.
Under general anesthesia and in the prone position his existing coronal scalp incision was used for wide open access to the back of his head. The prominent and irregular ridge of bone along the nuchal ridge was easily identified and reduced by a high-speed handpiece and rotary burr. At the same time the parietal bone above it was reduced as well as the parietal eminences at the sides. Such burin reduction of the skull creates a large amount of bone dust during its execution.
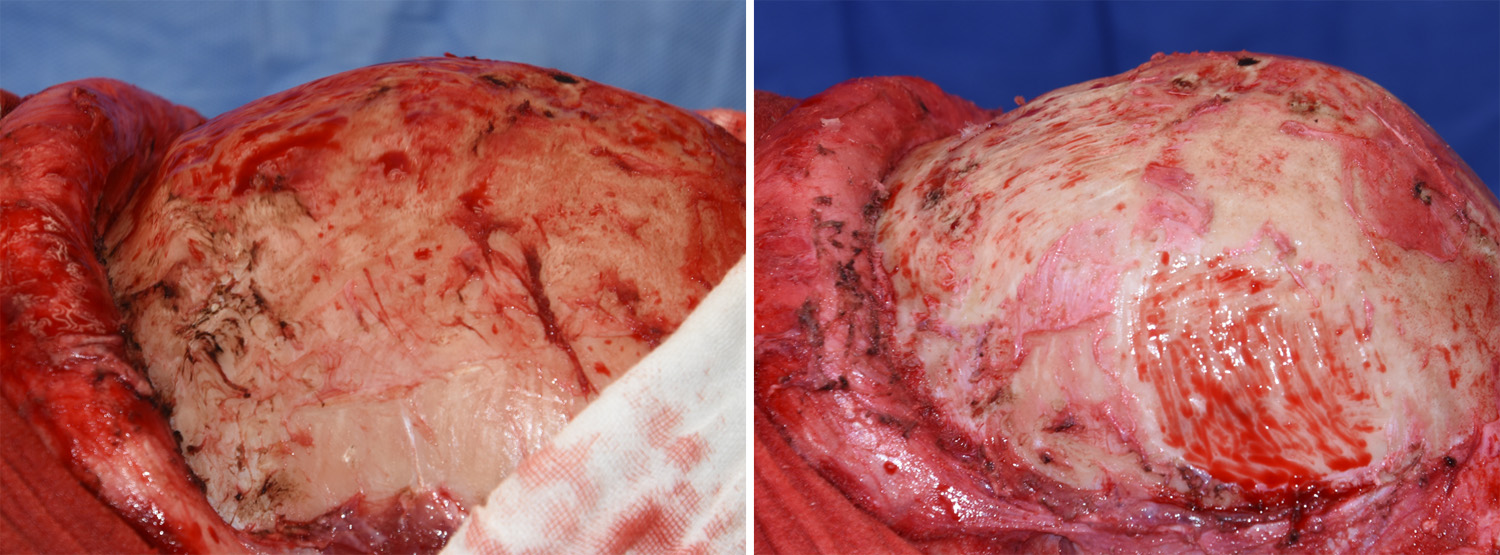
 The amount of nuchal ridge/occipital reduction could be appreciated in a side view comparison. Such an extensive amount of reduction can only be permitted by being able to use an existing full coronal scalp incision.
The amount of nuchal ridge/occipital reduction could be appreciated in a side view comparison. Such an extensive amount of reduction can only be permitted by being able to use an existing full coronal scalp incision.
Highlights:
1) The most commonly request are for skull reduction is the back of the head.
2) Back of the head protrusions can be caused by occipital knobs, nuchal ridge prominences, asymmetries or an overall generalized bony protrusion.
3) Occipital bone reduction is primarily done by a high-speed burring technique.
Dr. Barry Eppley
Indianapolis, Indiana