

Background: The size of one’s head is subject to a variety of normative values such as a circumferential measurement and percent of total body size. But regardless of numbers, the person’s interpretation of their head size is what is most aesthetically important. For those concerned about their head size, some people see their head size as too big while other see their head size as too small. Operations do exist for making the head size smaller or bigger but size increases can be greater than head size reduction.
While the head is composed of multiple regions (frontal, temporal, parietal, occipital and sagittal), creasing an overall head enlargement requires coverage of most of them. This near complete skull augmentation effect can only be done through a custom implant process. (skull helmet type implant) This allows an implant to be designed in a smooth fashion with tapered edges in which the various thicknesses over the different head zones can be precisely controlled.
Two very important preoperative head enlargement implant considerations are how large can the implant be both in design and scalp tolerance. Due to manufacturing limitations a total skull implant can not extend below a circumferential line drawn around that of the brows. This is so because it is important to avoid undercuts in its design. Also my experience has shown that large skull implants, unless they have a first stage scalp expansion procedure, can not usually exceed 200ccs in volume as the scalp will be too tight to close over them.
Case Study: This young make was bothered by the size of his head even though he had a full head of curly hair. He sought an overall head size enlargement change.
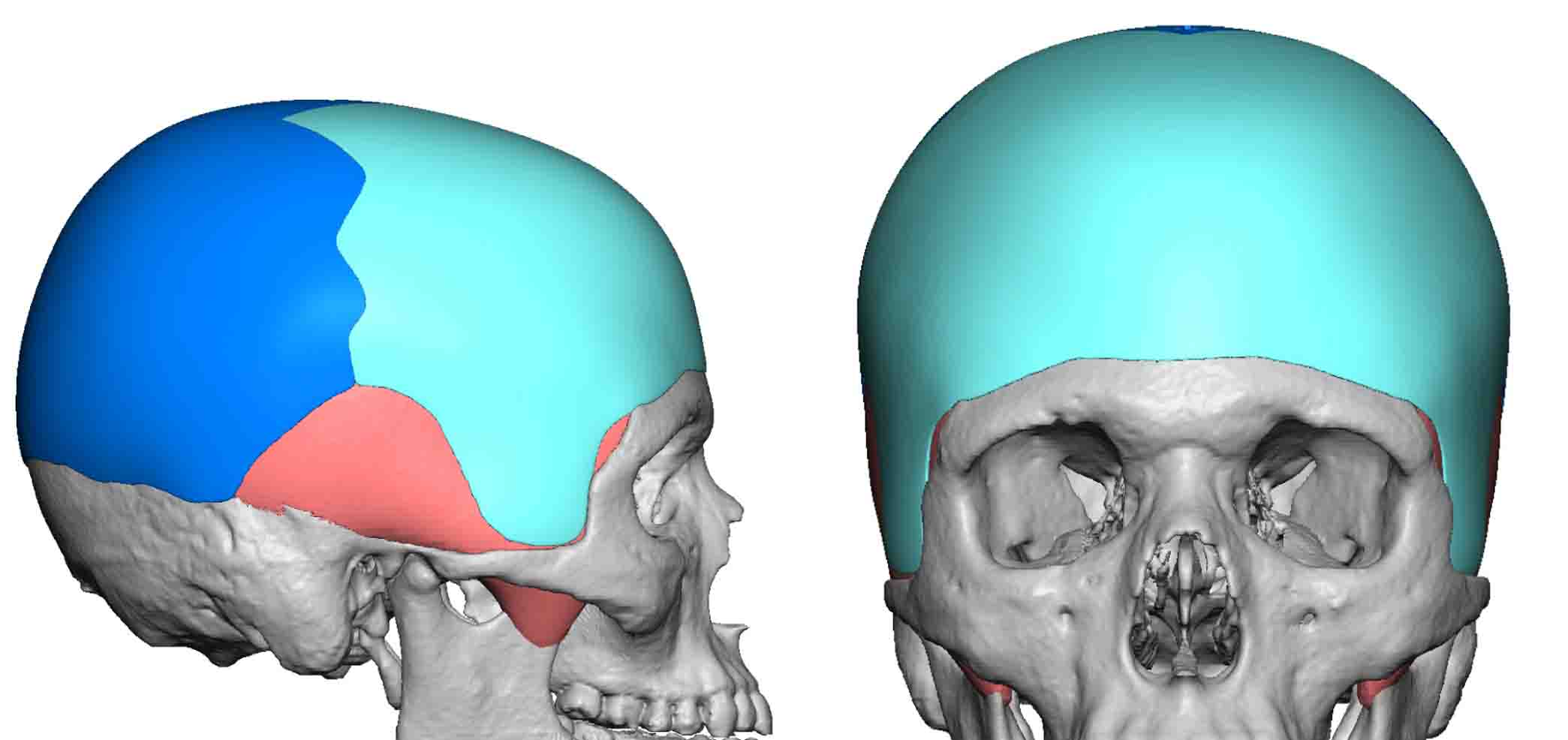
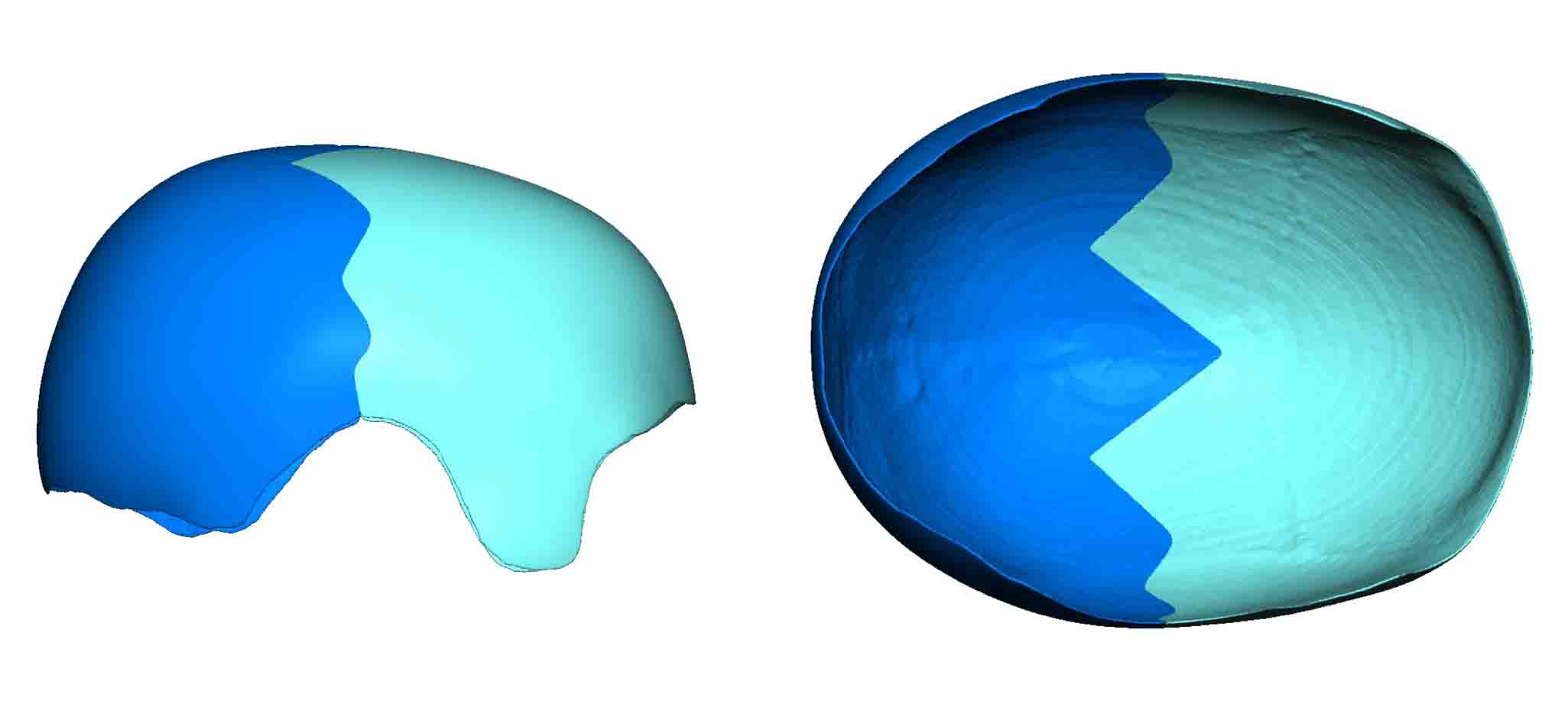 Using a 3D CT scan, a total custom skull implant was designed and manufactured in two pieces with an irregular sawtooth interdigitating connecting pattern. How low the implant design can extend both in the frontal, occipital and temporal regions are important considerations. Such an implant design is essentially a skull ‘helmet’.
Using a 3D CT scan, a total custom skull implant was designed and manufactured in two pieces with an irregular sawtooth interdigitating connecting pattern. How low the implant design can extend both in the frontal, occipital and temporal regions are important considerations. Such an implant design is essentially a skull ‘helmet’.
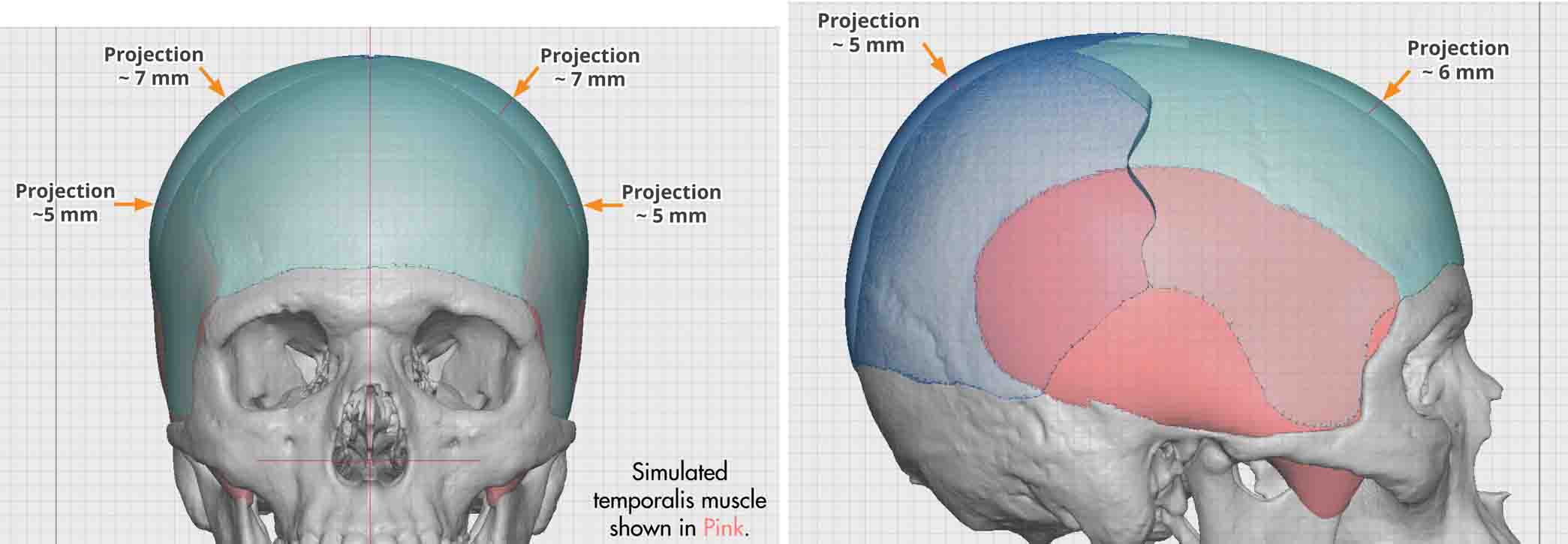 The thickest part of the skull implant was no more than 7mms with a total volume of 205ccs.
The thickest part of the skull implant was no more than 7mms with a total volume of 205ccs.

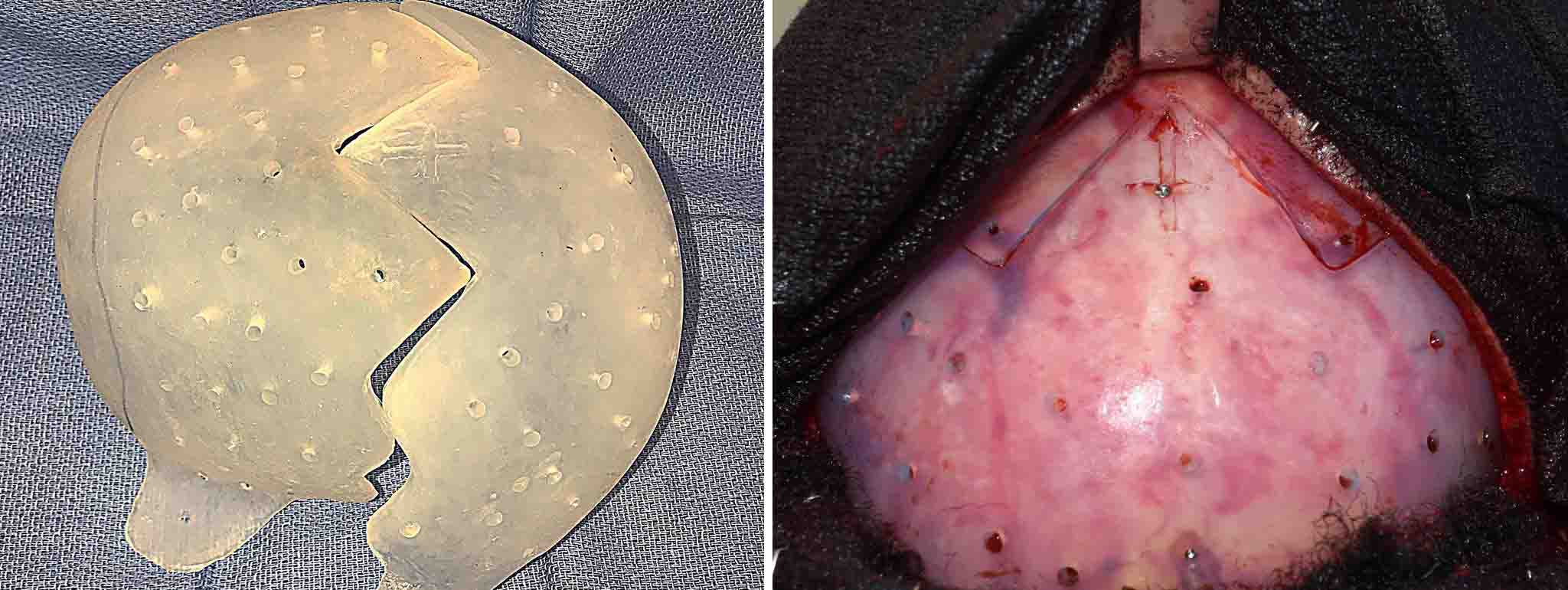 Under general anesthesia a subtotal corornal scalp incision was made halfway between the front and back of the head at the level of the ears. The scalp incision extended only 2 cms below the temporal lines. Subperioseal dissection was done on the bone areas and dissection on top of the deep temporalis fascia along the sides. Each half of the implant was used to size the front and back pockets and then inserted and assembled. The two umlaut halfs were secured along their seams with screws on each side.
Under general anesthesia a subtotal corornal scalp incision was made halfway between the front and back of the head at the level of the ears. The scalp incision extended only 2 cms below the temporal lines. Subperioseal dissection was done on the bone areas and dissection on top of the deep temporalis fascia along the sides. Each half of the implant was used to size the front and back pockets and then inserted and assembled. The two umlaut halfs were secured along their seams with screws on each side.
Whether one needs a first stage scalp expansion depends on how thick the implant design needs to be. While skull implants are designed by measurements of various areas, the key to whether the implant can be successfully placed is ultimately a volumetric one. When an implant covers such a large surface area it is an overall enlargement effect than is more profound than any single thickness measurement would suggest. Depending upon the patient’s natural scar elasticity it is prudent to keep the implant volume below 200ccs to ensure competent scalp closure and uncomplicated postoperative healing.
Highlights:
1) Custom skull implants can be done to cover most of the skull’s surface for an overall head enlargement effect.
2) Large skull implants must be made in two pieces due to manufacturing and incisional length restrictions.
3) Large skull implants up to 200cc in volume can be placed without prior scalp expansion.
Dr. Barry Eppley
Indianapolis, Indiana