

Background: The size of one’s head or skull is largely genetically driven unless there are congenital brain or skull deformities involved. Head sizes vary greatly amongst all people and even amongst gender, race and geographic location. There is no known intellectual differences between the broad normal range of head sizes that occur.
The interpretation of one’s head size, like many physical features, is open to personal interpretation. But there are people who truly do have a small overall head size which they interpret as aesthetically inadequate. Hair may do a lot to hide it but even with that coverage some people may still feel ‘inadequate’. They not infrequently have a history of being told they have a ‘peanut head’ amongst other unflattering commentaries.
It is now possible to change the size of ones head due to advances in computer design technology as well as the historic use of scalp tissue expansion. Using the patient’s 3D CT scan a near total skull implant can be designed with control of its perimeter routine as well as various material thicknesses. With the placement of such a large surface area implant under the scalp, an important question becomes whether the overlying scalp can adequately stretch to accommodate it. In most total skull implants the desire for a noticeable change almost always means the native scalp is not adequate and most be preoperatively stretched first. To no surprise the smaller the head the tighter the overlying scalp is.
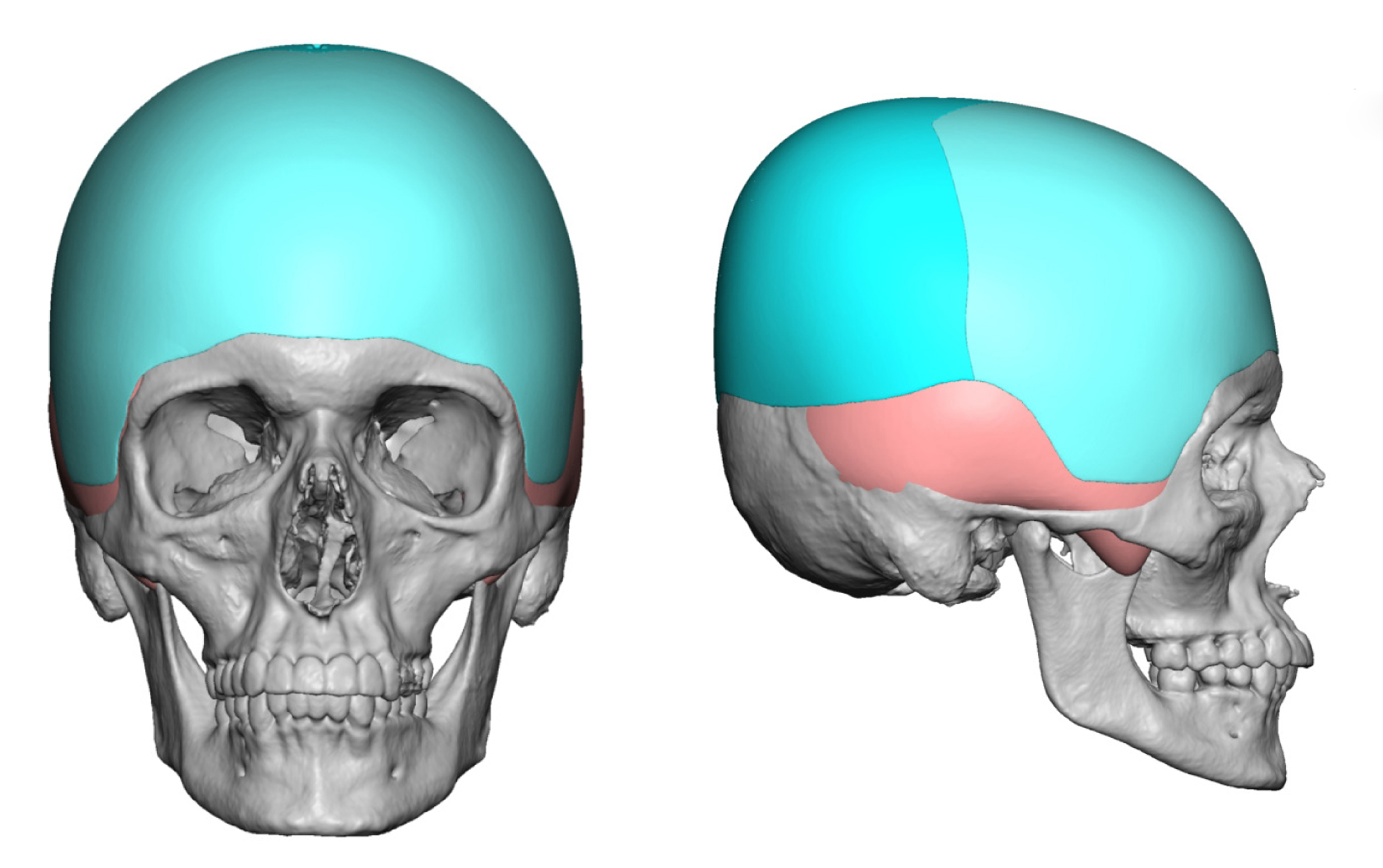
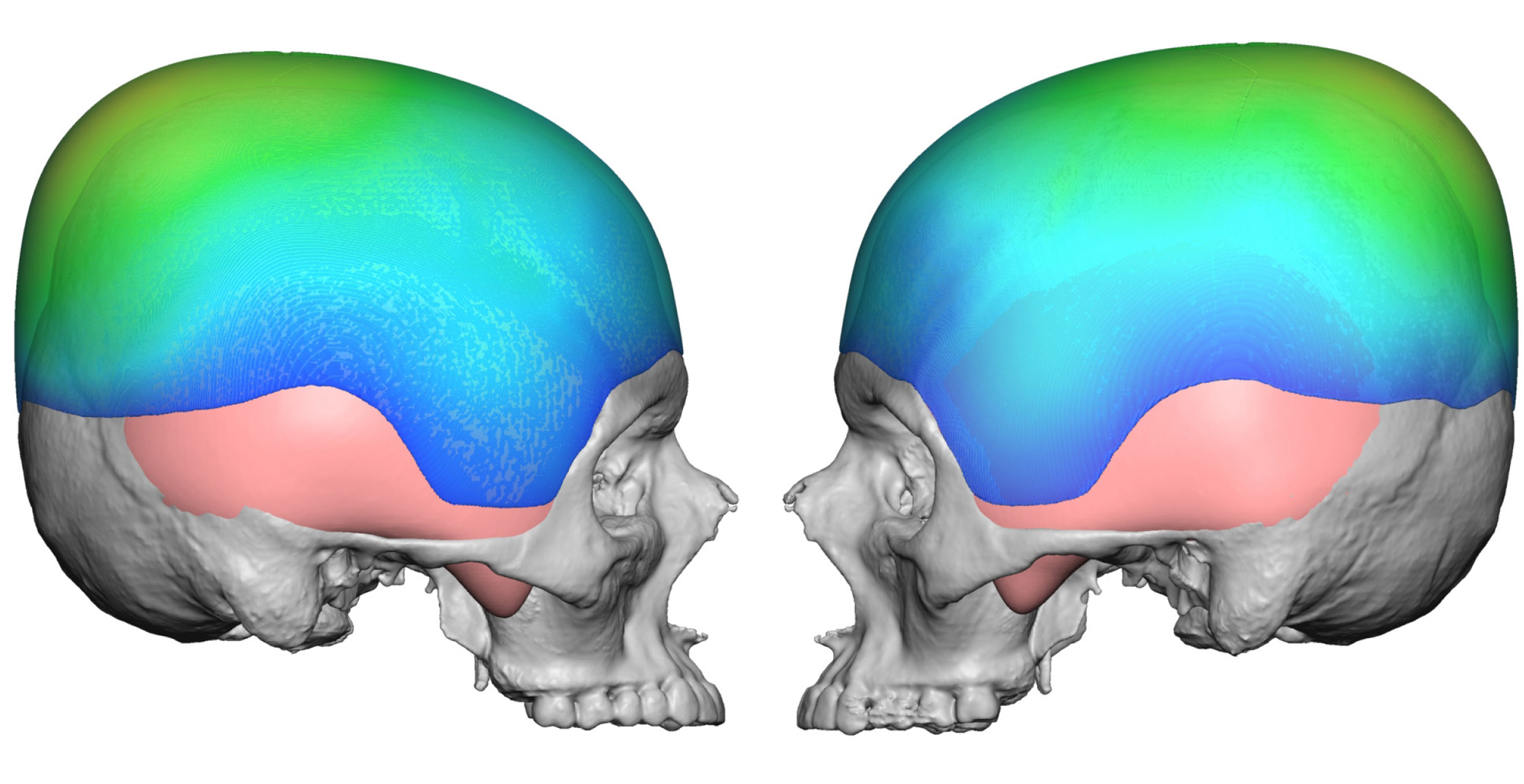 Case Study: This young male was bothered by his small head size and wanted an overall head size increase. Using his 3D CT scan a front to back and side to side skull implant was designed with average thicknesses across the top of the head from 8 to 9mms and in the crown area of 12mms. It extended anteriorly from the brow bone break to just above the nuchal ridge in the back. Along the sides it extended to the zygomatic arches in the temporal area and above the ears on its way to the back. Its total implant volume was 267ccs.
Case Study: This young male was bothered by his small head size and wanted an overall head size increase. Using his 3D CT scan a front to back and side to side skull implant was designed with average thicknesses across the top of the head from 8 to 9mms and in the crown area of 12mms. It extended anteriorly from the brow bone break to just above the nuchal ridge in the back. Along the sides it extended to the zygomatic arches in the temporal area and above the ears on its way to the back. Its total implant volume was 267ccs.
Because of the dimensions of the implant and his tight thinner scalp, a first stage scalp tissue expander was placed with a buried port above the right ear. He manually inflated it at home over a 5 week period to 250ccs. The day before the implant surgery an additional 25ccs was injected into it.
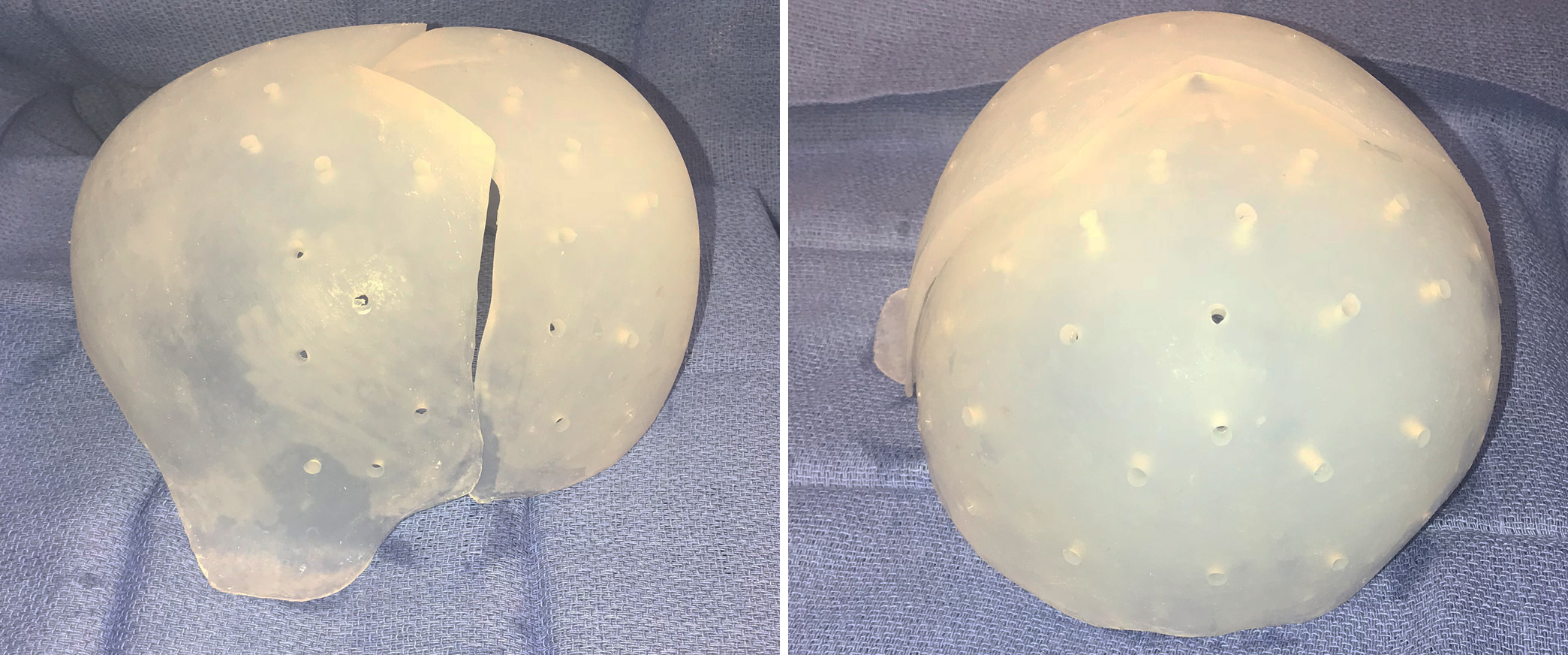 Under general anesthesia his skull implant surgery was performed through a hemi-coronal scalp incision that was limited to between the temporal lines across the top of his head. Total scalp elevation was done from this incision and the implant was inserted in two separate pieces, back first and then the front half. Keys to its placement are ensuring that the thin edges around the entire perimeter were unfurled and laying properly. It was also important to ensure that both pieces of the implant were centered along the patient’s sagittal midline and was aided in doing so using the compass marker on the implant.
Under general anesthesia his skull implant surgery was performed through a hemi-coronal scalp incision that was limited to between the temporal lines across the top of his head. Total scalp elevation was done from this incision and the implant was inserted in two separate pieces, back first and then the front half. Keys to its placement are ensuring that the thin edges around the entire perimeter were unfurled and laying properly. It was also important to ensure that both pieces of the implant were centered along the patient’s sagittal midline and was aided in doing so using the compass marker on the implant.
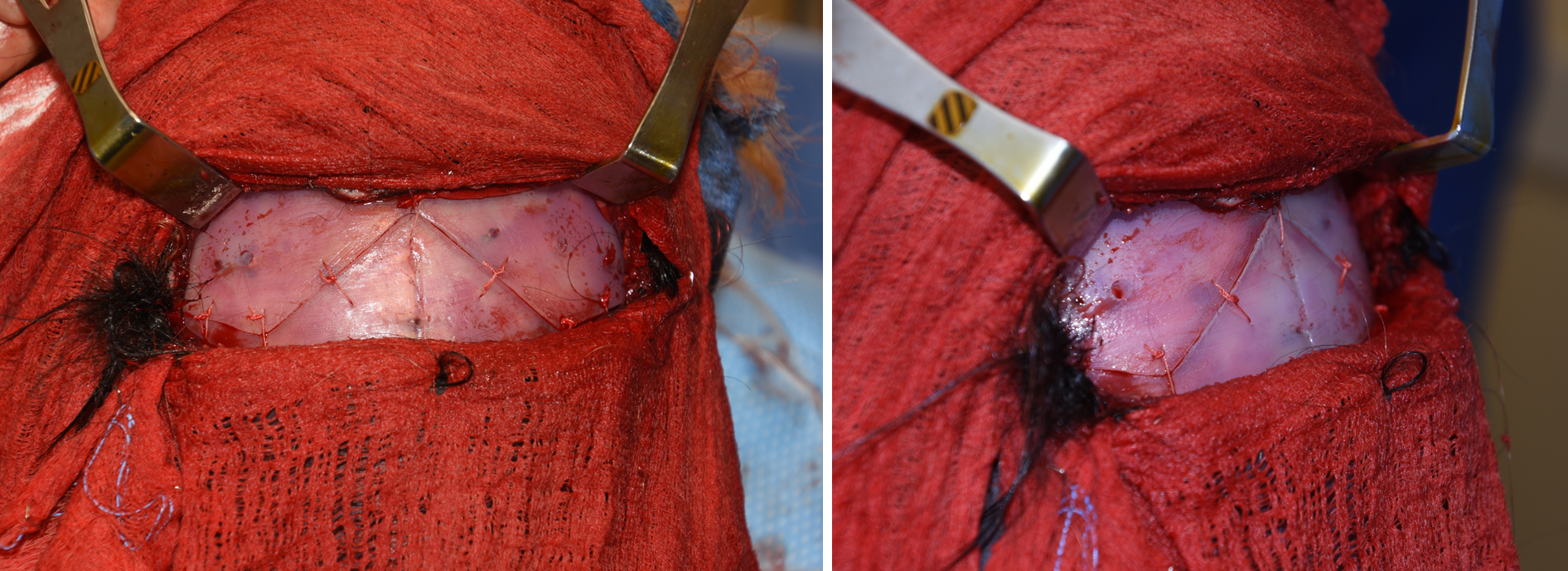
Intraoperative Suture Assembly of Large Custom Skull Implant Dr Barry Eppley IndianbapolisThe two pieces of the skull implant were initially sutured together with permanent sutures to bring together both sides of the implant along the saw tooth designed seam.
Intraoperative Screw Assembly of Large Custom Skull Implant Dr Barry Eppley IndianapolisOnce the skull implant was reassembled in place with a tight seam and centrally aligned, 2.0mm self-drilling screws were placed in a staggered fashion on both sides of the implant across its top surface.
 Significant skull enlargement can be done using a two-stage surgical process incorporating a temporal inflatable scalp expansion device followed by the placement of a large two-piece custom skull implant.
Significant skull enlargement can be done using a two-stage surgical process incorporating a temporal inflatable scalp expansion device followed by the placement of a large two-piece custom skull implant.
Highlights:
1) The natural boundary (size) of the overall skull can be enlarged through near total implant coverage.
2) Such large custom skull implants requite a two-piece design and placement technique.
3) When the total volume of the skull augmentation exceeds 150 ccs, a first stage scalp tissue expander is needed.
Dr. Barry Eppley
Indianapolis, Indiana