

Background: Microtia is a well known congenital ear deformity where the external ear has variable amounts of underdevelopment. It is not that rare of a facial deformity affecting about 1 in 10,000 births. While it can occur in both ears, it more commonly affects one side of which it occurs far more frequently on the right side.
Microtia is almost always treated, at least in the U.S., in childhood. Its reconstruction is done by two basic methods in children, a completely autologous rib graft method and a combined synthetic ear framework covered by an autologous fascial flap-skin graft. There are surgical advocates for each ear reconstruction method and each one has its own distinct advantages and disadvantages. In children the use of a synthetic ear framework and rib graft methods is probably about equally divided.
Adult microtia is very rare in the U.S. as almost all cases get some form of treatment as a child. It is becoming more prevalent with the growing number of immigrants who did not have access to plastic surgery care in their country of origin. But regardless of the nationality of the adult, the tilt in ear reconstruction favors the use of a synthetic framework method as it avoids a rib graft scar and the unpredictability of how well adult rib cartilage can be shaped.
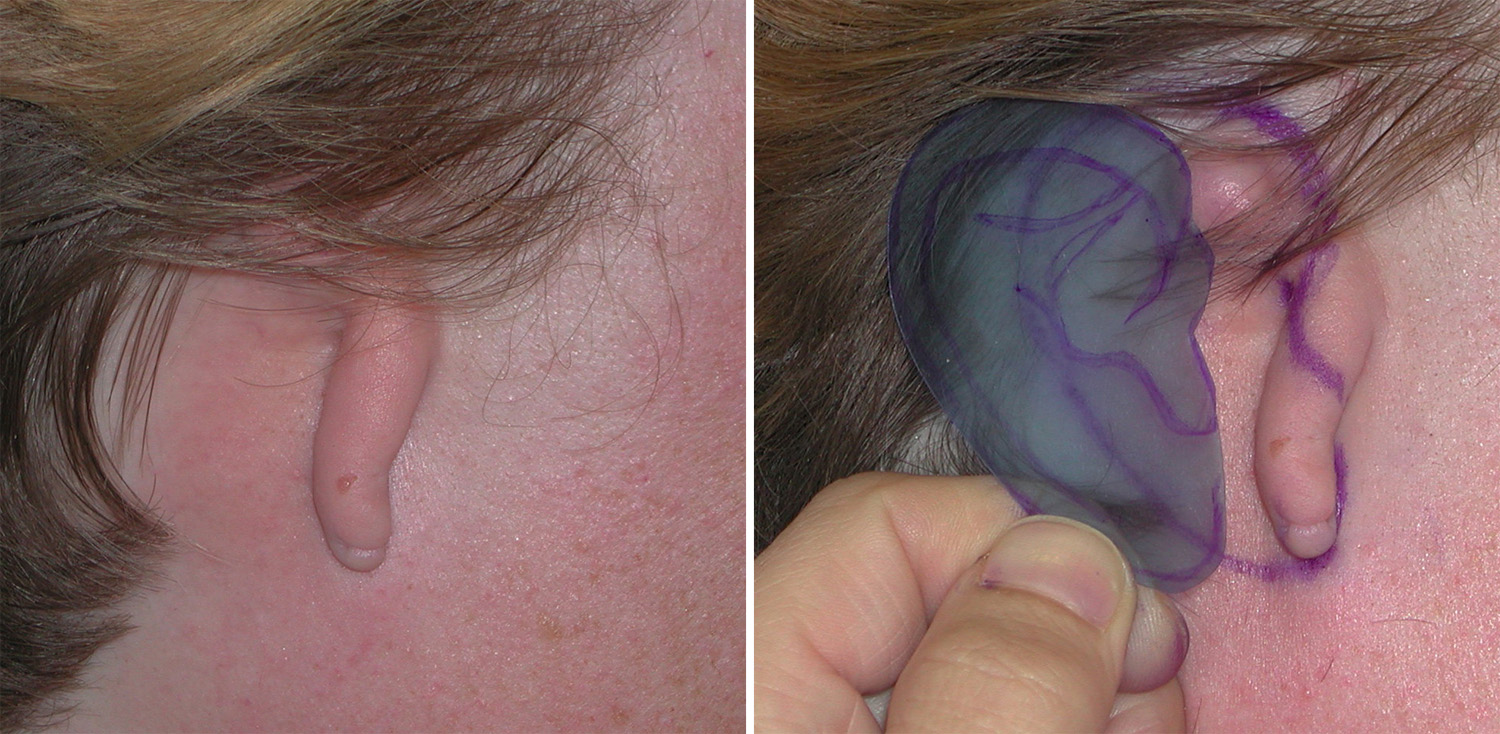 Case Study: This 40 year-old female presented with an isolated type 2 right microtia that had never been treated. The remainder of her face was unaffected. A template was made of the opposite left ear and transferred to the affected right side for optimal angulation and height of the ear reconstruction.
Case Study: This 40 year-old female presented with an isolated type 2 right microtia that had never been treated. The remainder of her face was unaffected. A template was made of the opposite left ear and transferred to the affected right side for optimal angulation and height of the ear reconstruction.

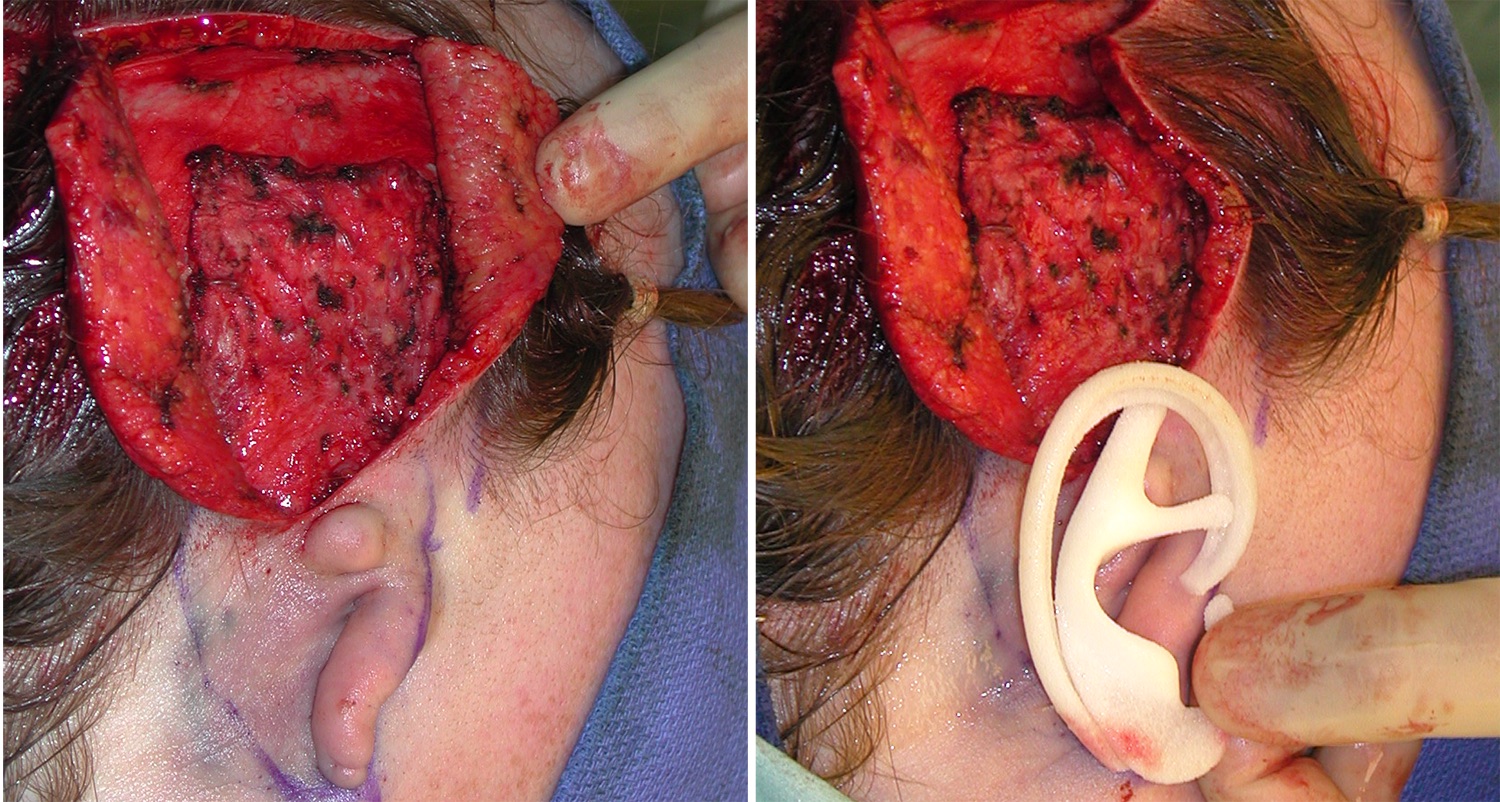 Under general anesthesia a vertical incision above the ear was made up into the temporal region. From this incisional access a temporals fascial flap (TPF) was raised from the temporal line downward maintaining the superficial temporal vessels as its vascular pedicle. A Medpor ear framework was used and placed into a subcutaneous pocket that contained the ear remnants on its outer surface.
Under general anesthesia a vertical incision above the ear was made up into the temporal region. From this incisional access a temporals fascial flap (TPF) was raised from the temporal line downward maintaining the superficial temporal vessels as its vascular pedicle. A Medpor ear framework was used and placed into a subcutaneous pocket that contained the ear remnants on its outer surface.
 Once the synthetic framework was placed, the temporalis fascial flap was brought down over and into the subcutaneous pocket to cover as much of the implant as possible. The superior part of the flap and implant was covered with a full-thickness skin graft. In a second stage procedure three months later, the residual elements on the skin were removed.
Once the synthetic framework was placed, the temporalis fascial flap was brought down over and into the subcutaneous pocket to cover as much of the implant as possible. The superior part of the flap and implant was covered with a full-thickness skin graft. In a second stage procedure three months later, the residual elements on the skin were removed.
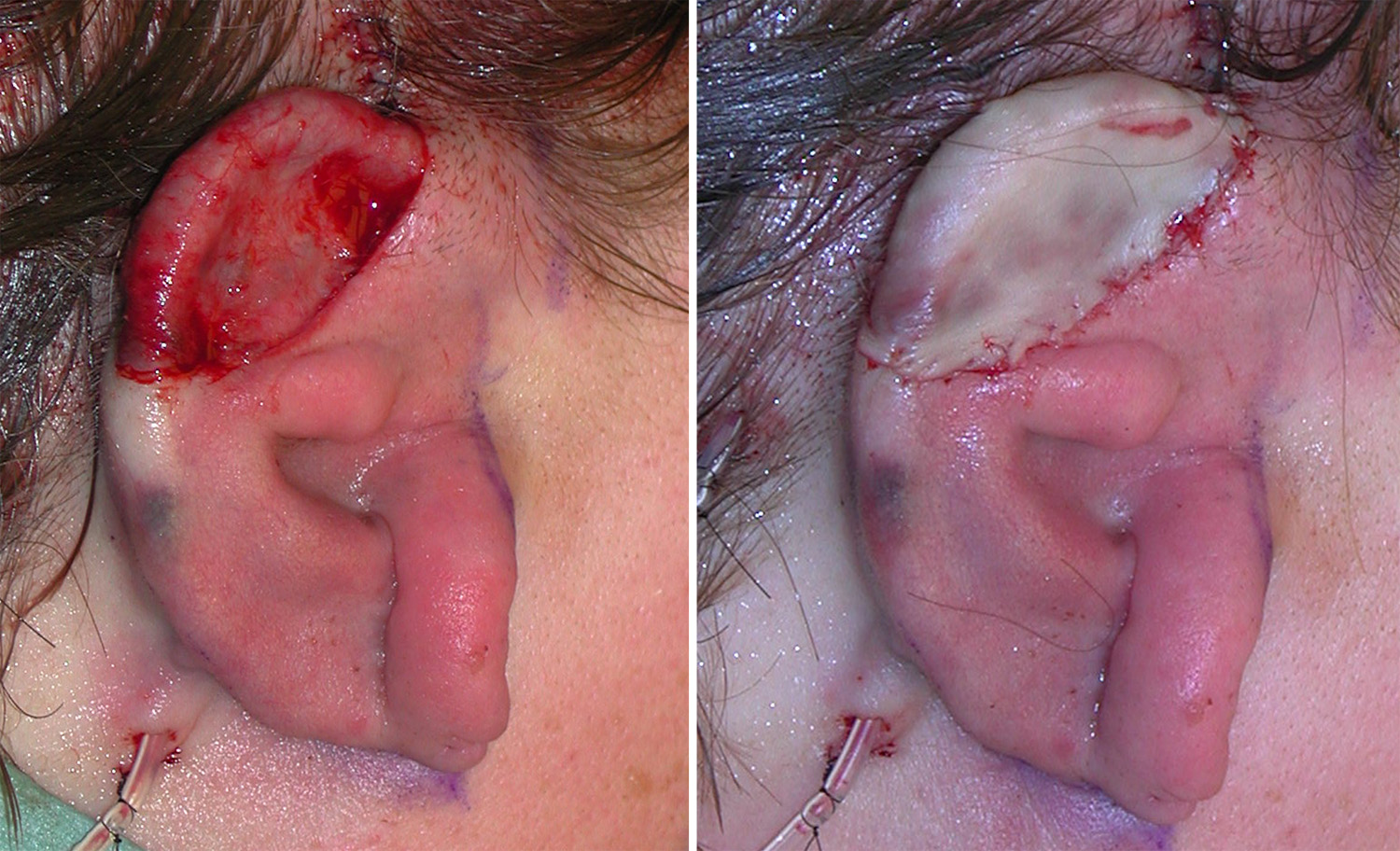
 When seen six months after the original framework and flap reconstruction, and three months after the remnant excisions, the shape of the ear reconstruction had good detail. The skin grafted area looked much whiter than the surrounding natural ear skin as would be expected.
When seen six months after the original framework and flap reconstruction, and three months after the remnant excisions, the shape of the ear reconstruction had good detail. The skin grafted area looked much whiter than the surrounding natural ear skin as would be expected.
In adult microtia reconstruction, an implant and autologous soft tissue coverage approach is preferred. It produces the best looking result due to the implant’s shape and often can be done in just one stage with simultaneous flap and skin graft outer coverage.
Highlights:
1) Adult microtia reconstruction is very uncommon in the U.S.
2) Adult ear reconstruction usually consists of a synthetic framework covered with a temporalis fascial flap and skin graft.
3) In adult females the temporal scar is less relevant than it is in many adult males for the peddled flap harvest.
Dr. Barry Eppley
Indianapolis, Indiana