

Background: Mant types of aesthetic breast ‘deformities’ present in the breast augmentation patient. Issues such as breast asymmetry, sagging, wide sternal spacing, lateralization of the breast round and horizontal nipple asymmetries are the most common. Each present their own challenges and potential aesthetic distractions from an ideal breast augmentation result.
One potential aesthetic nipple concern in the breast augmentation candidate is that of the inverted nipple. This is where the nipple lacks projection and indents inward rather than outward. Its relevance in this anesthetic operation is whether it will be improved by the placement of an implant or not. While it is fair to assume that in most cases it will not, then the opportunity to do a concurrent inverted nipple correction at the same time as breast implant placement exists.
While the inverted nipple externally often appears to be an homogenous deformity it is not. Different types of nipple inversions are well known based on their cause as well as the degree of retraction. This is pertinent to the type of inverted nipple repair needed as well as whether the pressure of an underlying implant will also be the solution to the inverted nipple. The key preoperative test as to whether an implant has any chance to improve nipple inversion is the ‘squeeze test’. If the nipple can be made to protrude by gentle pressure on the surrounding areola, implant placement MAY provide an effective solution to it.
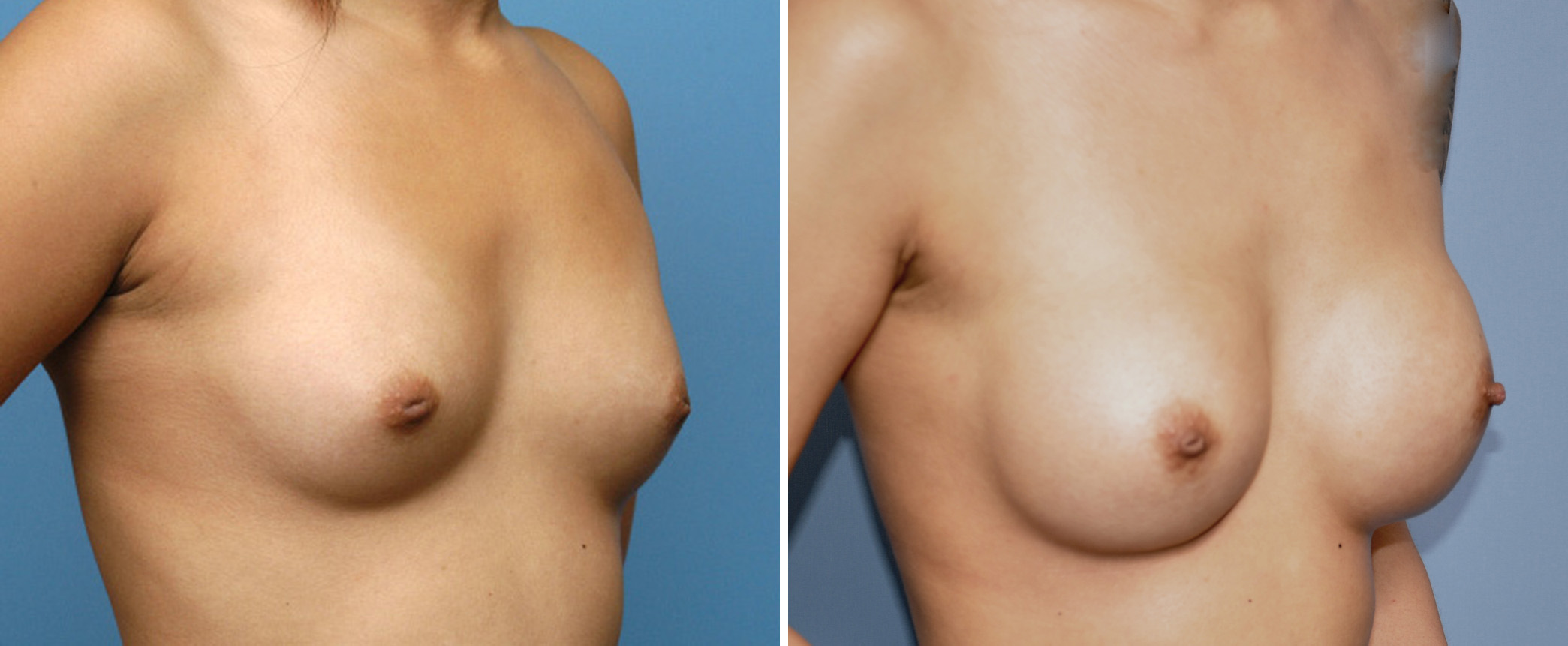
Case Study: This young Asian female presented for breast augmentation who also had congenital nipple inversion. She had never been pregnant but could make the nipple protrude out by pressure on the surrounding areola or breast mound.
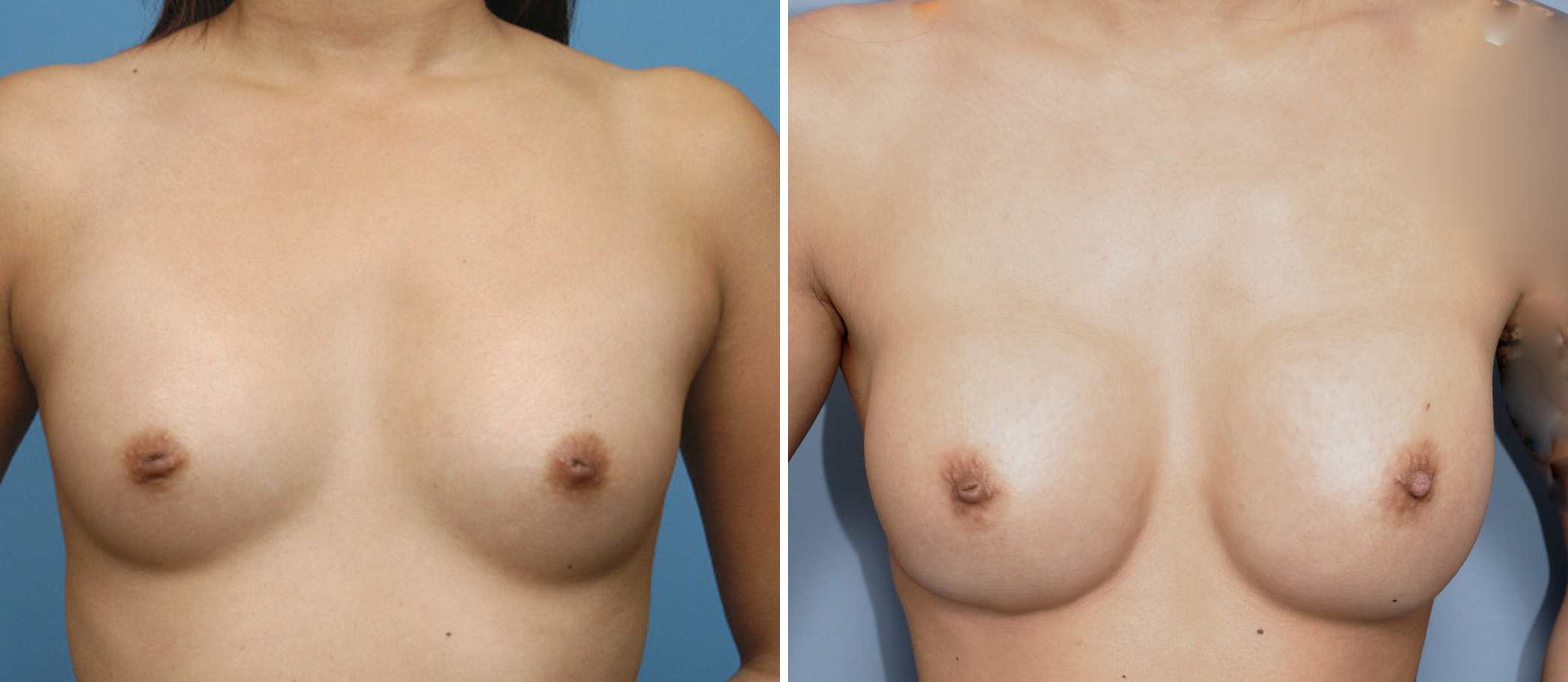 Under general anesthesia and through a transaxillary approach, 300cc silicone moderate plus profile implants were placed in a partial submuscular position. In so doing the nipples inversions were simultaneously corrected on the operative table.
Under general anesthesia and through a transaxillary approach, 300cc silicone moderate plus profile implants were placed in a partial submuscular position. In so doing the nipples inversions were simultaneously corrected on the operative table.
When seen six weeks after surgery the nipples remained protruding outward.
 Most congenital nipple inversions are more severely contracted and do easily retract due to fibrosis. The nipple either never developed or has fibrous bands that tether the nipple inward. Conversely acquired nipple inversion occurs due to pregnancy and breastfeeding. Such nipple inversions are less severe because they are acquired and originally had natural protrusion. The squeeze test is a preoperative method that provides insight into whether the pressure of an underlying implant can push out the nipple inversion. If so then one can take a wait and see approach as between the implant placement and the breast mound swelling, the nipple usually does come out of a positive preoperative squeeze test was positive. If not then one should plan on a concurrent inverted nipple repair technique employing release and possible interpositional graft.
Most congenital nipple inversions are more severely contracted and do easily retract due to fibrosis. The nipple either never developed or has fibrous bands that tether the nipple inward. Conversely acquired nipple inversion occurs due to pregnancy and breastfeeding. Such nipple inversions are less severe because they are acquired and originally had natural protrusion. The squeeze test is a preoperative method that provides insight into whether the pressure of an underlying implant can push out the nipple inversion. If so then one can take a wait and see approach as between the implant placement and the breast mound swelling, the nipple usually does come out of a positive preoperative squeeze test was positive. If not then one should plan on a concurrent inverted nipple repair technique employing release and possible interpositional graft.
Highlights:
1) Some women that present for breast augmentation have nipple inversion, either congenital or pregnancy-induced.
2) Whether breast augmentation alone has the potential to solve nipple inversion can be determined by preoperative testing.
3) For inverted nipples that fail the preoperative test, concurrent inverted nipple repair at the time of breast augmentation can be done.
Dr. Barry Eppley
Indianapolis, Indiana