

Background: The well known sagittal split ramus osteotomy of the mandible provides a change in the position of the tooth-bearing portion of the lower jaw. It can move the lower jaw forward or back in the sagittal direction. It is not infrequently done in conjunction with a sliding genioplasty, another sagittal type osteotomy that is isolated to just that of the chin. Done together the amount of forward projection of the lower jaw can be considerable.
As the jaw is brought forward, the most common movement for the sagittal split procedure, it may adversely affect the appearance of the jaw angle. This shape change can occur due to some bone loss from partial devascularization, a change in its actual position when fixed back to the distal bone segment, or can appear to be different because of the other changes to the jawline. (pseudo jaw angle deficiency) Such jaw angle changes usually are 3D in nature having both a horizontal and vertically deficient appearance
Despite the many facial advantages offered by the sagittal split osteotomy, it does not provide any width to the lower jaw. It also can not create any vertical lengthening of the jaw angles. In fact there are no osteotomies or bony type movements that can do so. Only implants can create true three dimensional augmentation to the jaw angles at the back of the jaw.
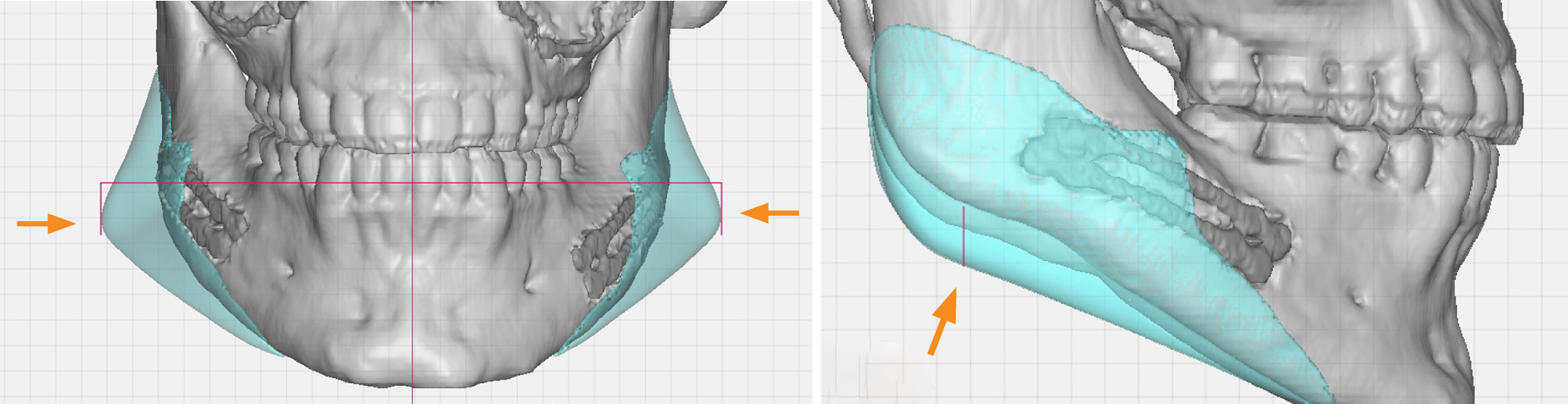 Case Study: This young male had a previous bimaxillary orhognathic surgery procedure which brought his face forward. While he was pleased with his chin projection he now felt that the back of his jaw was deficient, lacking both width and vertical length. Using a 3D CT scan custom jaw angle implants were designed to create a more visible and pronounced back of the jaw that was compatible with his amount of chin projection. The indwelling plates used to fixate the sagittal split osteotomies could be seen crossing across the original split proximal and distal segments.
Case Study: This young male had a previous bimaxillary orhognathic surgery procedure which brought his face forward. While he was pleased with his chin projection he now felt that the back of his jaw was deficient, lacking both width and vertical length. Using a 3D CT scan custom jaw angle implants were designed to create a more visible and pronounced back of the jaw that was compatible with his amount of chin projection. The indwelling plates used to fixate the sagittal split osteotomies could be seen crossing across the original split proximal and distal segments.

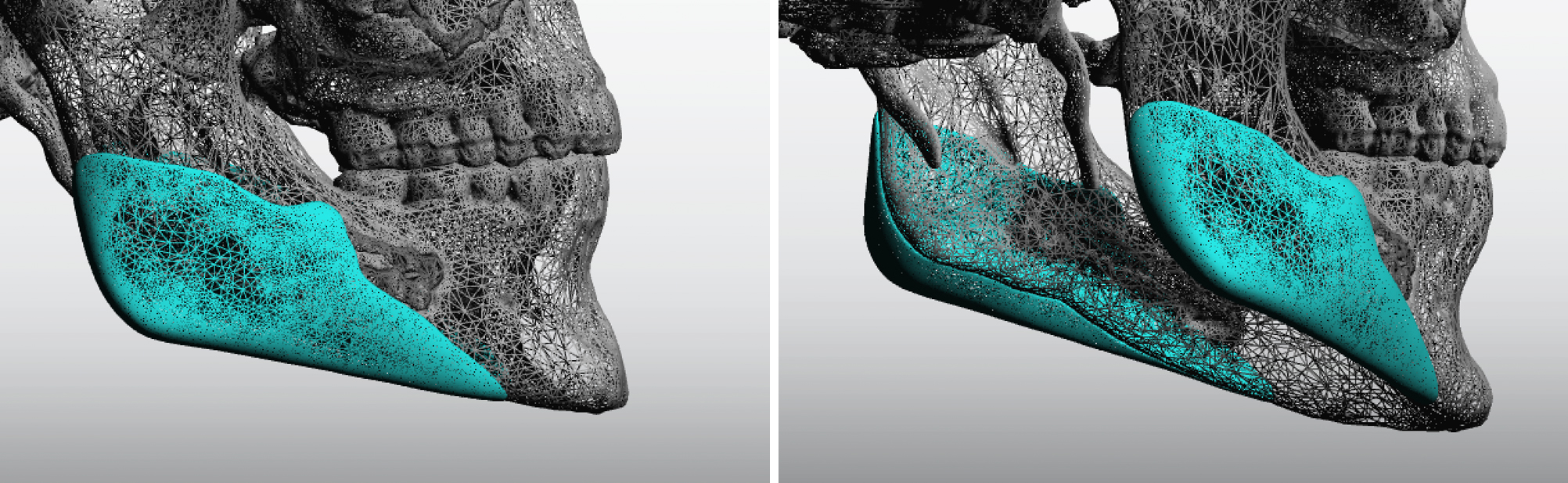 Three-dimensional imaging rotation of the custom jaw angle implant designs show how it creates stronger jaw angles by expanding the existing ramus bone boundaries. This also creates a smoother and straight inferior border jawline between the angle and the chin with a lower mandibular plane angle.
Three-dimensional imaging rotation of the custom jaw angle implant designs show how it creates stronger jaw angles by expanding the existing ramus bone boundaries. This also creates a smoother and straight inferior border jawline between the angle and the chin with a lower mandibular plane angle.
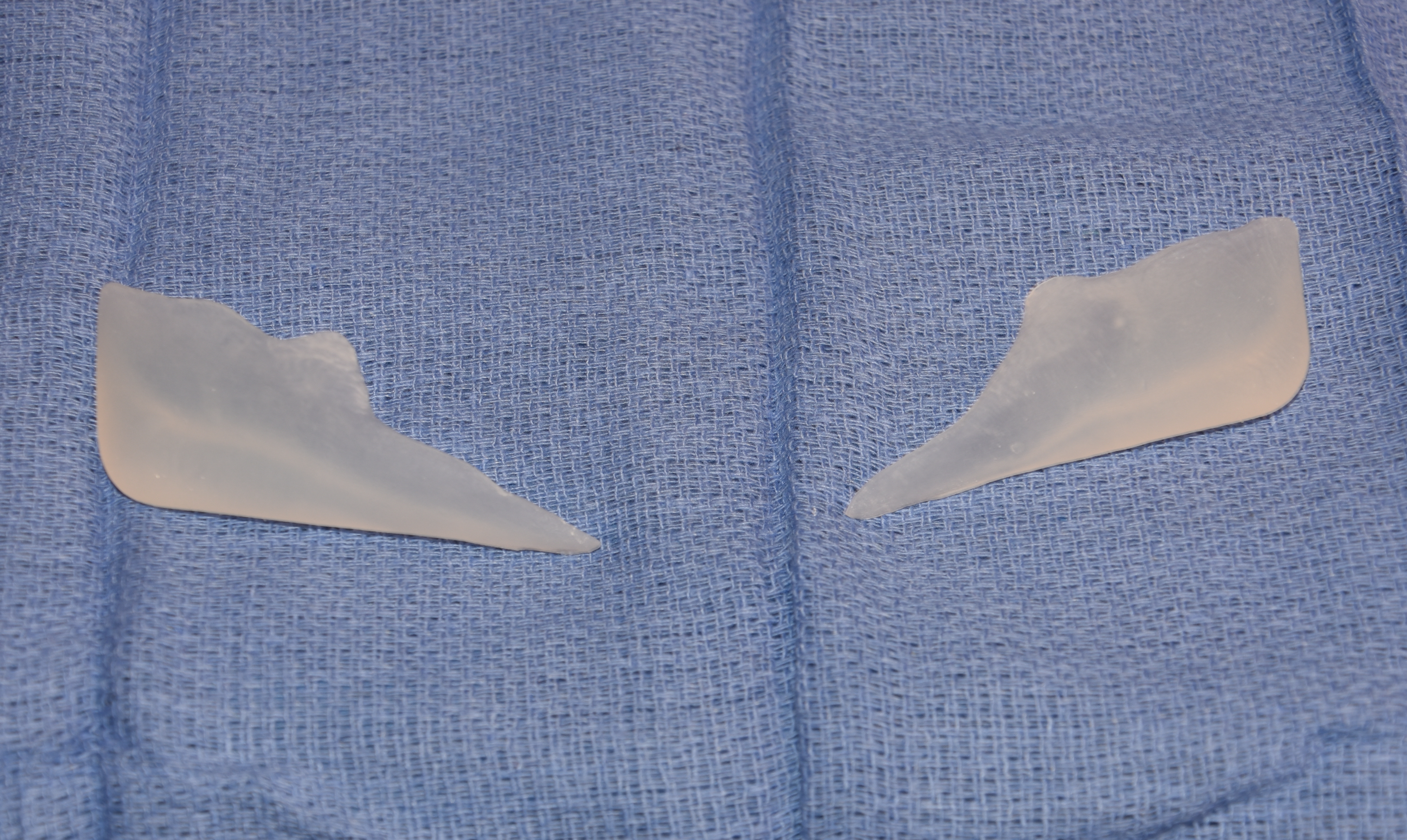 Under general anesthesia and through existing posterior vestibular intraoral scars, the jaw angles were exposed and the pterygomasseteric sling carefully elevated along the inferior border from the angle point to an anterior point just below the mental nerve. The implants were inserted and secured by double screw fixation. The placement of the fixation screws was quite challenging given the large surface area covered by existing plate which was largely overgrown with bone.
Under general anesthesia and through existing posterior vestibular intraoral scars, the jaw angles were exposed and the pterygomasseteric sling carefully elevated along the inferior border from the angle point to an anterior point just below the mental nerve. The implants were inserted and secured by double screw fixation. The placement of the fixation screws was quite challenging given the large surface area covered by existing plate which was largely overgrown with bone.
This case represents what is a pseudo jaw angle deficiency. This means that the jaw angles have not actually lost shape but moving the tooth-bearing part of the jaw and the chin forward now makes them look aesthetically ‘deficient’. This is not unlike the patient who gets a chin implant and then later feels that his jawline is deficient or weak behind it. Given the need for vertical lengthening and the inevitable asymmetries of the jaw angles that almost always exists after a sagittal split osteotomy, custom jaw angle implants are needed for the best chance of the paired back of the jaw bone to be evenly augmented.
Case Highlights:
1) Jaw angle deformities can occur after sagittal split ramus osteotomies, either by bone alteration or creating a pseudo deficiency.
2) Pseudo deficiencies of the jaw angle after jaw advancement are often have a significant vertical component as well as a horizontal one.
3) Custom jaw angle implants are needed in these cases which are made from a 3D CT scan.
Dr. Barry Eppley
Indianapolis, Indiana