

Background: The deficient or deformed back of the head is the most common aesthetic skull deformity. Lack of sufficient projection and a more convex contour are the main reasons patient seek a surgical solution to these concerns. Such aesthetic skull concerns, in my experience, occur equally in women and men. Women find that they have to try and use their hair to hide the lack of occipital shape. Conversely it comes to men’s attention in most cases because they either shave their heads or have a closely cropped hair style.
What has made the augmentation of the back of the head, and just about all skull augmentations, a reliable and effective procedure is the use of custom implants. Such a skull contouring technique allows the precise shaping and design of the augmentation material to be done before surgery and also permits a smaller scalp incision to be used for placement.
While a custom skull implant can be designed to any shape and dimensions, that does always mean it can be successfully placed. The natural flexibility of the scalp or how much it can stretch controls the size of the implant that can be placed under it. This is particularly true when the incisional access is more limited and the elevation of the scalp tissues off of the bone is also more restrictive. Unlike a full coronal scalp incision where wide undermining of the scalp flaps can be done in either direction and larger implants can be placed, the desire in most aesthetic skull augmentations is for a more limited scalp incision. This means that in most patients, the maximal thickness of the implant at its central projection should be under 15mm.
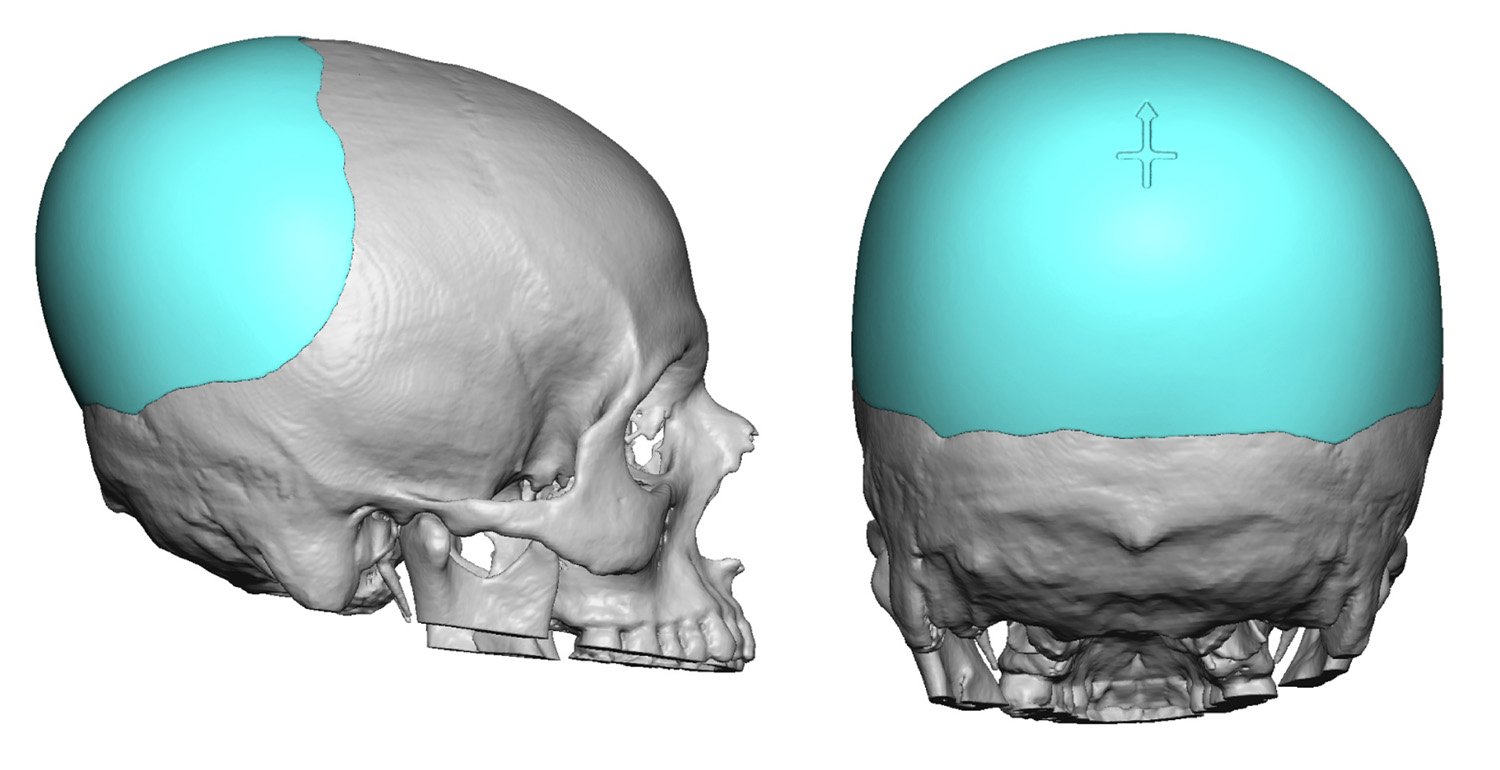 Case Study: This 30 year female felt that the back of his head lacked projection particualrly more in the upper crown area. Even though she currently had a longer hair, this was not always her preferred hair style. Using a 3D CT scan a custom occipital skull implant was designed to augment her crown area with a central thickness of 12 mms.
Case Study: This 30 year female felt that the back of his head lacked projection particualrly more in the upper crown area. Even though she currently had a longer hair, this was not always her preferred hair style. Using a 3D CT scan a custom occipital skull implant was designed to augment her crown area with a central thickness of 12 mms.
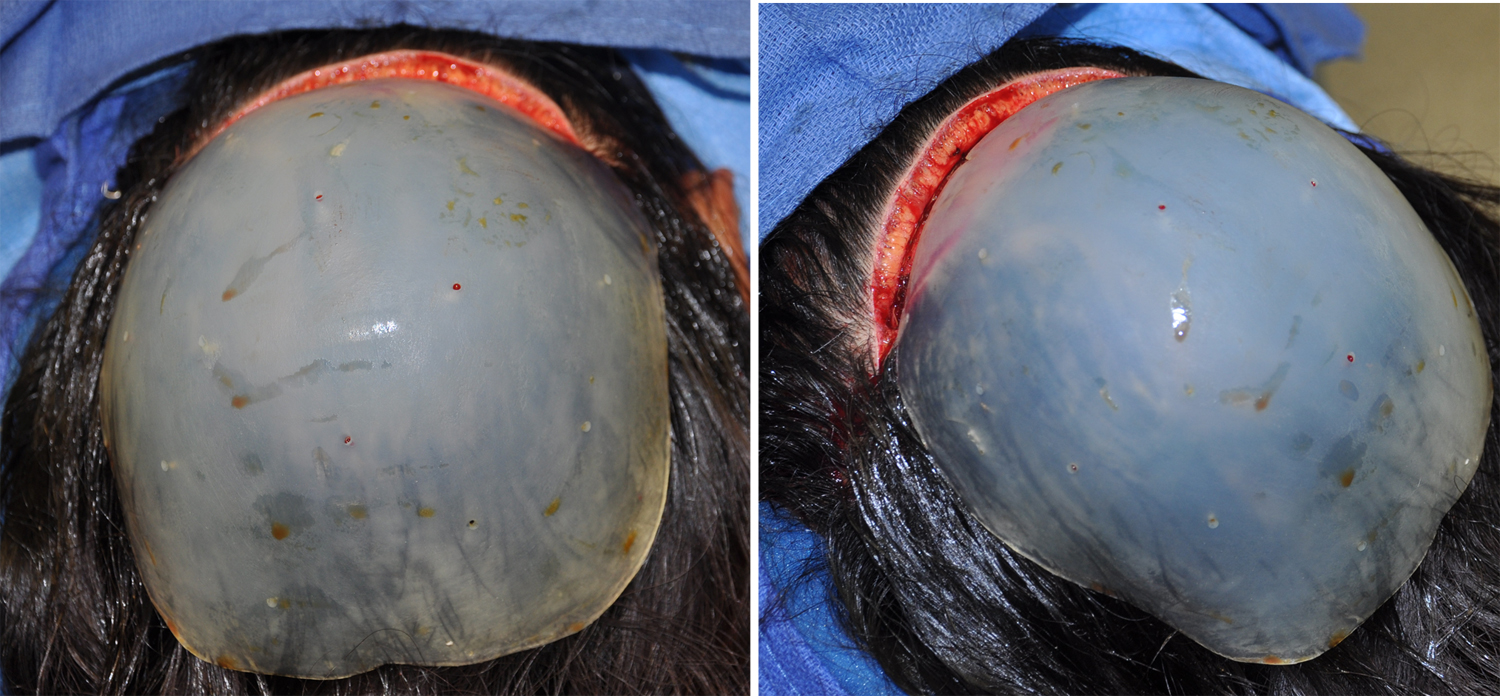 Under general anesthesia and in the prone position, a 9 cm long mid-occipital scalp incision was made. Wide subperiosteal undermining was done into which the implant, which had been intraoperatively prepared with multiple perfusion holes, was placed. Given that the implant was much wider than 9 cms, this required it to be folded on insertion and then unfolded once under the scalp flap. The tightness of the overlying scalp tissues and the precision fit of the implant on the bone does not usually require any form of implant fixation. The incision was closed with dissolveable sutures. No hair is ever shaved for the placement of skull implants.
Under general anesthesia and in the prone position, a 9 cm long mid-occipital scalp incision was made. Wide subperiosteal undermining was done into which the implant, which had been intraoperatively prepared with multiple perfusion holes, was placed. Given that the implant was much wider than 9 cms, this required it to be folded on insertion and then unfolded once under the scalp flap. The tightness of the overlying scalp tissues and the precision fit of the implant on the bone does not usually require any form of implant fixation. The incision was closed with dissolveable sutures. No hair is ever shaved for the placement of skull implants.
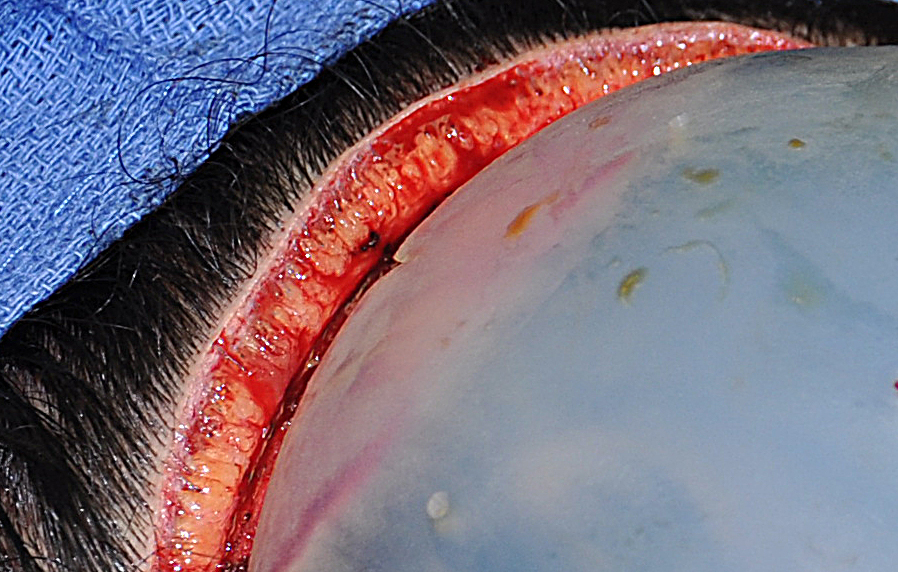 One interesting aspect of custom skull implants, that is often asked by patients, is their potential impact on the hair follicles. As seen in this closeup picture the location of the hair follicles, which much deeper than most people realize, is still much more superficial than the implant. Of the five scalp layers the hair follicles are in the second layer with the implant is under the fifth layer.
One interesting aspect of custom skull implants, that is often asked by patients, is their potential impact on the hair follicles. As seen in this closeup picture the location of the hair follicles, which much deeper than most people realize, is still much more superficial than the implant. Of the five scalp layers the hair follicles are in the second layer with the implant is under the fifth layer.
Highlights:
- The flat back of the head occurs in either a complete projection deformity or more or a crown deficiency.
- A custom occipital skull implant is the best method for any form of occipital skeletal deficiency or asymmetry.
- The thickness and surface area coverage of custom skull implants is controlled by one’s scalp flexibility.
Dr. Barry Eppley
Indianapolis, Indiana