

Background: Skull shape deformities are not typically perceived as an aesthetic problem. But just because they are not common does not mean they are not just as significant to someone who has it nor that they can not be improved satisfactorily. There are a wide range of aesthetic skull deformities that affect its entire length from the forehead back to where the neck muscles attach to the bottom end of the skull.
One of the most common aesthetic skull deformities is that of the flat back of the head. Occurring from either in utero or neonatal positioning the back of the head can suffer a non-neurologic deformation, ending up with a variety of flattened shapes. This flattening may or may not be associated with compensatory widening of the parietal bones creating flaring or widening in the back with the flat spot in between the two sides. (known as brachycephaly) While this can occur in anyone under the right circumstances, the Asian population is particularly prone to occipital flattening. This may be due to inherent development patterns in which front to back skull growth is naturally shorter.
While to the uninformed, flatness on the back of the head may be perceived as trivial and easily covered by hair. Nothing is further from the truth to someone who has it. I have heard many stories from patients abut the time and effort they put into styling their hair to camouflage it or from men who constantly wear hats to keep it covered. For some men what was once something they could feel, losing their hair begins a process of exposure of their flat back of the head and can serve as tbe the stimulus to seek a surgical solution.
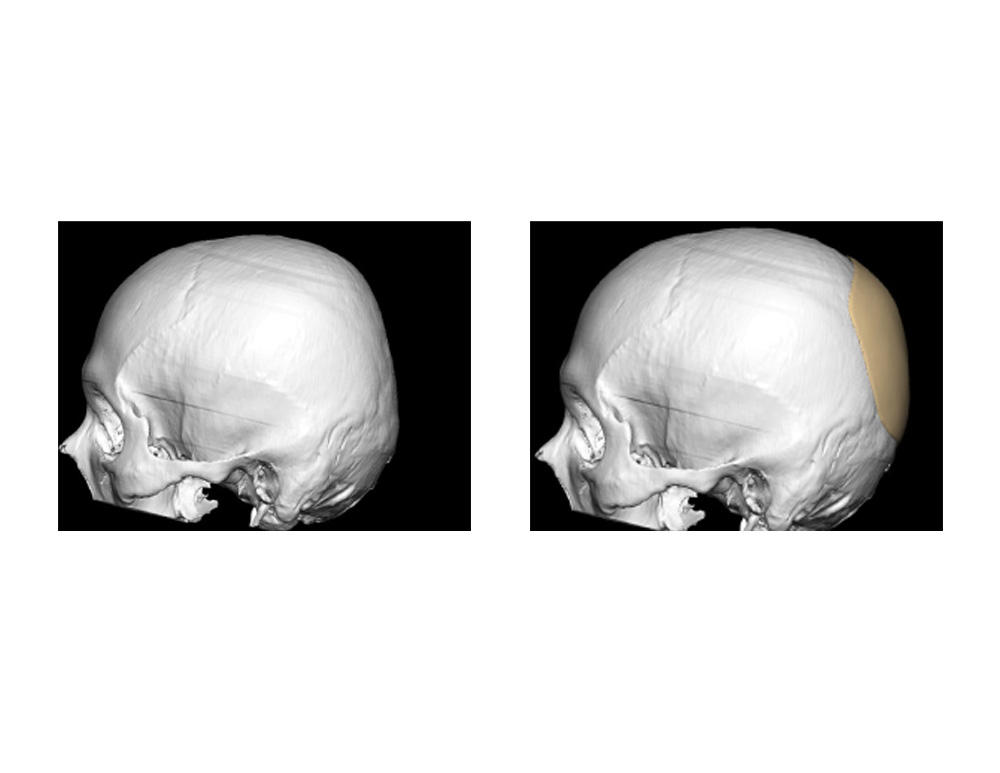 Case Study: This 42 year-old Asian male had always been bothered by the flat spot on the back of his head. He routinuely spent time with gel products making his hair stand up in the back for camouflage. The flatness of the back of his head could be seen in a 3D CT scan with a severe drop-off from the top of the skull down. From this scan, a custom silicone implant was designed to cover the flat area with a central thickness of 8mms. He also had occipital asymmetry with the right side having a greater degree of flatness in which the design compensated by more material on that side.
Case Study: This 42 year-old Asian male had always been bothered by the flat spot on the back of his head. He routinuely spent time with gel products making his hair stand up in the back for camouflage. The flatness of the back of his head could be seen in a 3D CT scan with a severe drop-off from the top of the skull down. From this scan, a custom silicone implant was designed to cover the flat area with a central thickness of 8mms. He also had occipital asymmetry with the right side having a greater degree of flatness in which the design compensated by more material on that side.
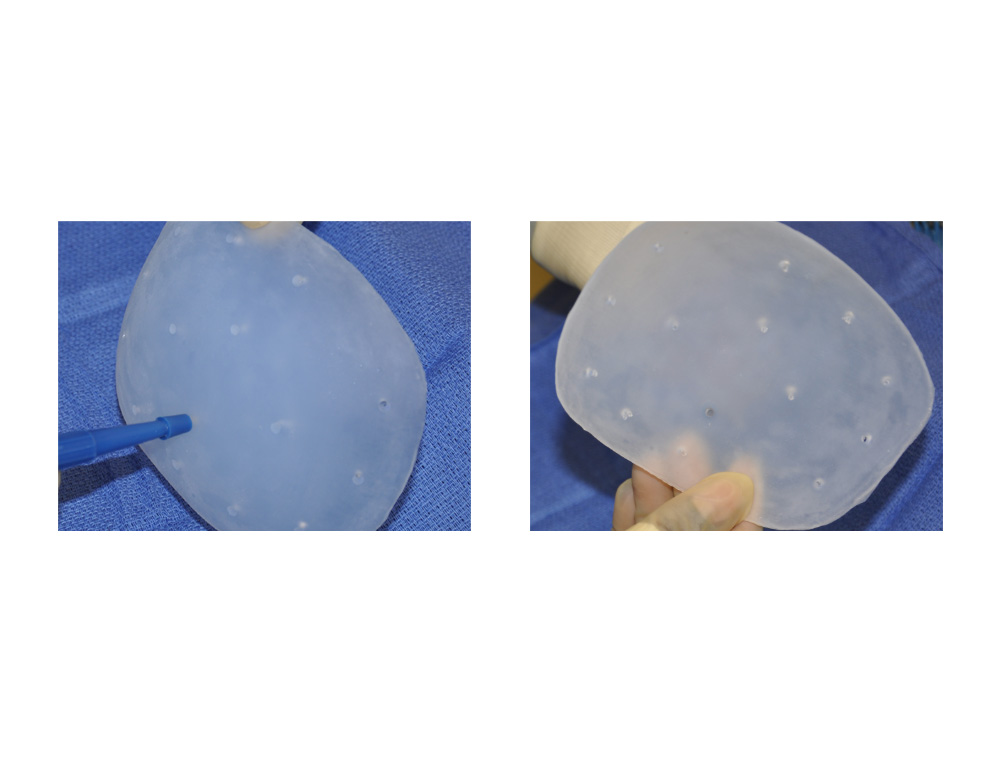
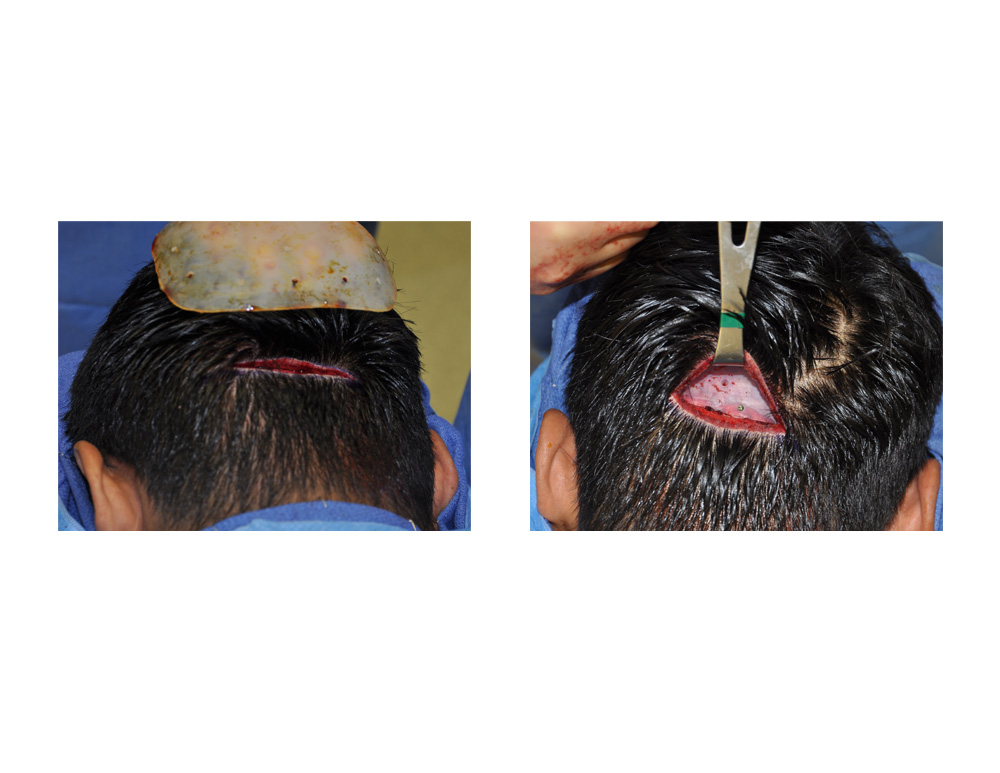 Under general anesthesia, he was turned into the padded prone position. A horizontal 4.5cm incision was made low in the occipital hairline just below the nuchal ridge. Dissection was done down to the bone and wide subperiosteal undermining was done with long curved dissectors beyond where the implant edges would be in a 270 degree radius from the incision. The implant was prepared by making multiple ‘perfusion holes’ through it with a 3mm dermal punch. It was then folded for insertion, unfolded once inside, positioned and then secured with a single 1.5mm self-tapping screw at its lower edge.
Under general anesthesia, he was turned into the padded prone position. A horizontal 4.5cm incision was made low in the occipital hairline just below the nuchal ridge. Dissection was done down to the bone and wide subperiosteal undermining was done with long curved dissectors beyond where the implant edges would be in a 270 degree radius from the incision. The implant was prepared by making multiple ‘perfusion holes’ through it with a 3mm dermal punch. It was then folded for insertion, unfolded once inside, positioned and then secured with a single 1.5mm self-tapping screw at its lower edge.
 The effects of the implant were immediate and no edge-transitions could be felt. The incision was closed in two layers with small resorbable sutures for the skin. He had some mild pain the first night but took no narcotic medications after the first 24 hours. He looked very ‘non-surgical’ the next day.
The effects of the implant were immediate and no edge-transitions could be felt. The incision was closed in two layers with small resorbable sutures for the skin. He had some mild pain the first night but took no narcotic medications after the first 24 hours. He looked very ‘non-surgical’ the next day.
Having performed occipital augmentation with various materials, there is no question that using a custom silicone implant is the simplest approach. By its prefabricated design and the smooth silicone material, it is also the most assured way to avoid any palpable edge transitions of the implant to the bone. The placement of perforating perfusion holes allows for multiple points of fibrous fixation that will ensure that the implant will never move or migrate despite its smooth surface. Such holes also prevent any flexing of the implant in an area like the back of the head where it encounters frequent pressure when laying. (although this is more likely to happen in a non-custom implant that does not have a perfect fit.
Case Highlights:
1) Augmentation for the flat back of the head can provide a significant aesthetic improvement.
2) A custom occipital implant made from the patient’s 3D CT provides the most accurate fit for the flat back of the head.
3) A custom implant can be placed through a low horizontal skin incision at the base of the neck, which may be particularly advantageous in men,
Dr. Barry Eppley
Indianapolis, Indiana