

Background: A flat back of the head, also known as occipital brachycephaly, is a not uncommon aesthetic skull shape concern. It may occur from the way one laid in utero, how they were positioned as an infant while sleeping or from a genetic tendency based on race. To those so afflicted with this skull shape deformity, they can go to great lengths to camouflage it using hair styles, hats and other concealing maneuvers.
The flat back of the head can be very effectively treated by occipital augmentation using various bone cements and implants. The incisional approach to place these skull augmentation materials can be either high up on the occiput just behind the vertex or low in the occiput just along the nuchal line. There are very few reasons for a long coronal incision with most of today’s implant materials.
But one fundamental principle of occipital augmentation is that there has to be enough scalp to accommodate the amount of ‘bone’ expansion required. The scalp tissues are fairly tight and there is a limit as to how much they can stretch with an immediate augmentation. It has been my experience that about 10mm to 15mms of central occipital expansion can be obtained with an immediate augmentation. More than that will require a scalp tissue expander to be placed before attempting implant placement. The expander only needs to be inflated to about the size of the occipital augmentation needed. Another reason for a first stage scalp expansion are scars and prior scalp tissue loss due to injury or previous surgery.
Case Study: This 41 year-old male had a very flat back of the head that had bothered him for years. He had two prior hair transplant procedures done using a strip harvest method in the low occipital region with a scar that wrapped around ear to ear. Using computer imaging predictions, it was determined that the amount of augmentation he needed was 15mms at the central occipital region. But given his prior hair transplant harvests his scalp was very tight and it was felt that even this amount of occipital augmentation could not be safely achieved.
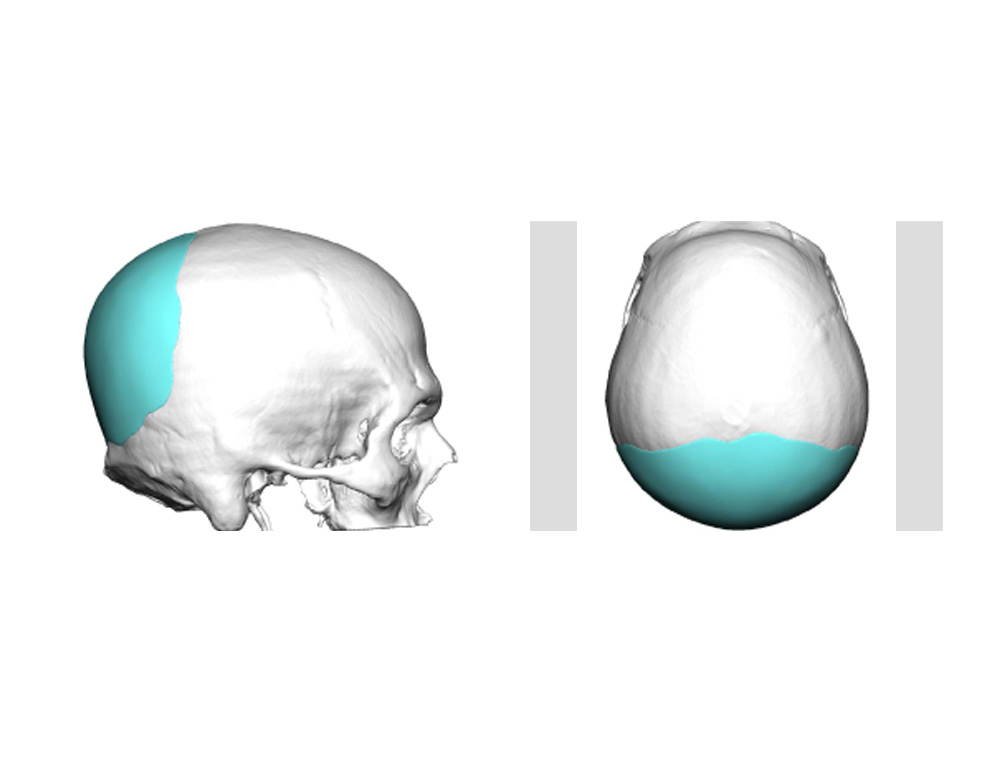
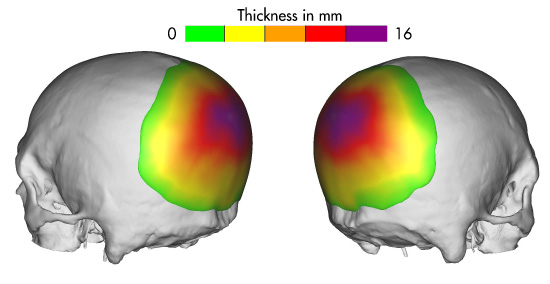 A first stage scalp tissue expander was placed through the central aspect of his hair transplant scar in the low occipital region. It was inflated at home slowly up to 100ccs over six weeks. In the interim, a 3D CT scan was used to create a custom occipital implant with 16mms of thickness in its central aspect.
A first stage scalp tissue expander was placed through the central aspect of his hair transplant scar in the low occipital region. It was inflated at home slowly up to 100ccs over six weeks. In the interim, a 3D CT scan was used to create a custom occipital implant with 16mms of thickness in its central aspect.
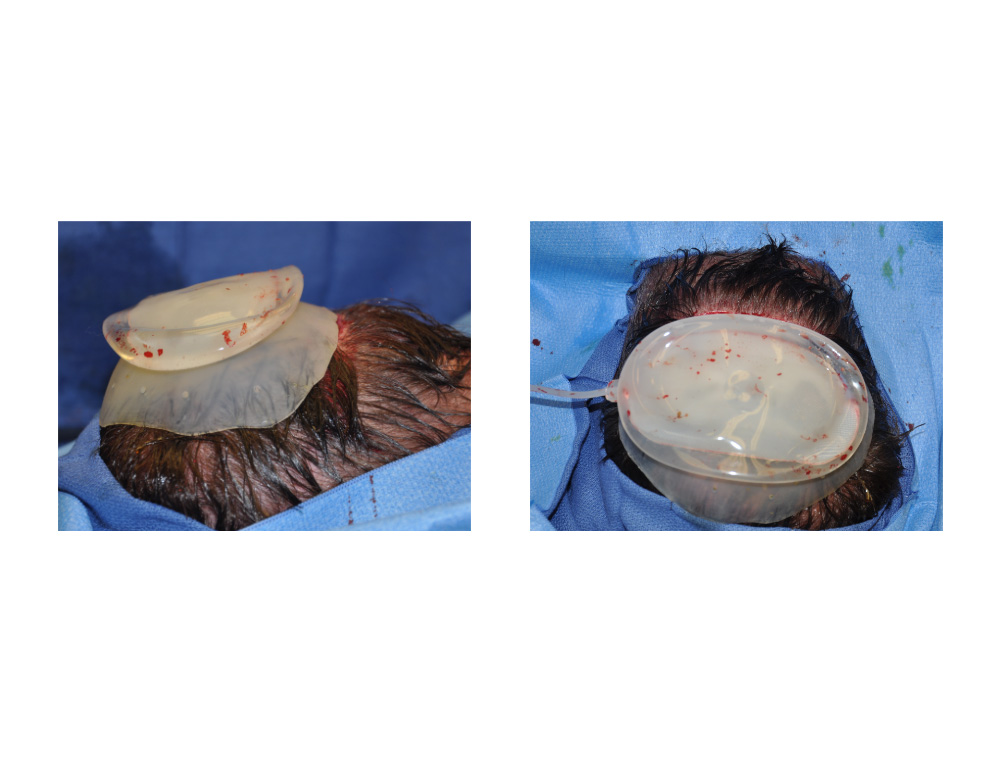
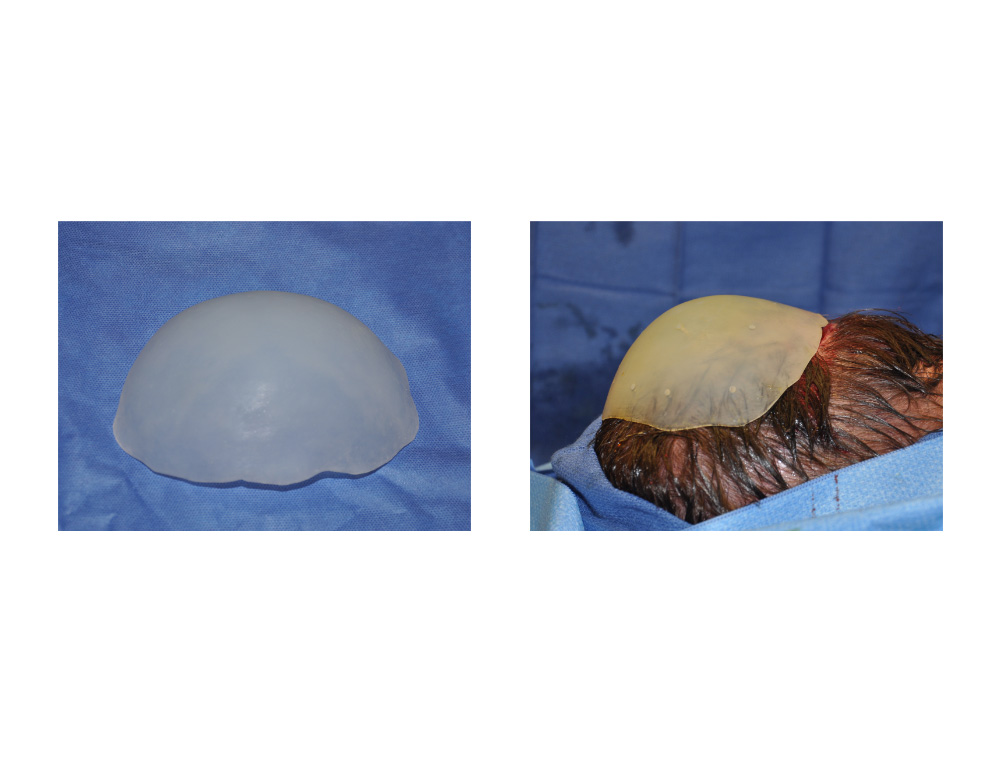 A second stage procedure was done through the same occipital incision. The tissue expander was removed and it could be seen that it matched fairly closely to the size of the occipital implant. The custom occipital silicone implant was perforated with a 2mm dermal punch throughout to create multiple perfusion holes. It was inserted through the incision, positioned and the incision closed.
A second stage procedure was done through the same occipital incision. The tissue expander was removed and it could be seen that it matched fairly closely to the size of the occipital implant. The custom occipital silicone implant was perforated with a 2mm dermal punch throughout to create multiple perfusion holes. It was inserted through the incision, positioned and the incision closed.
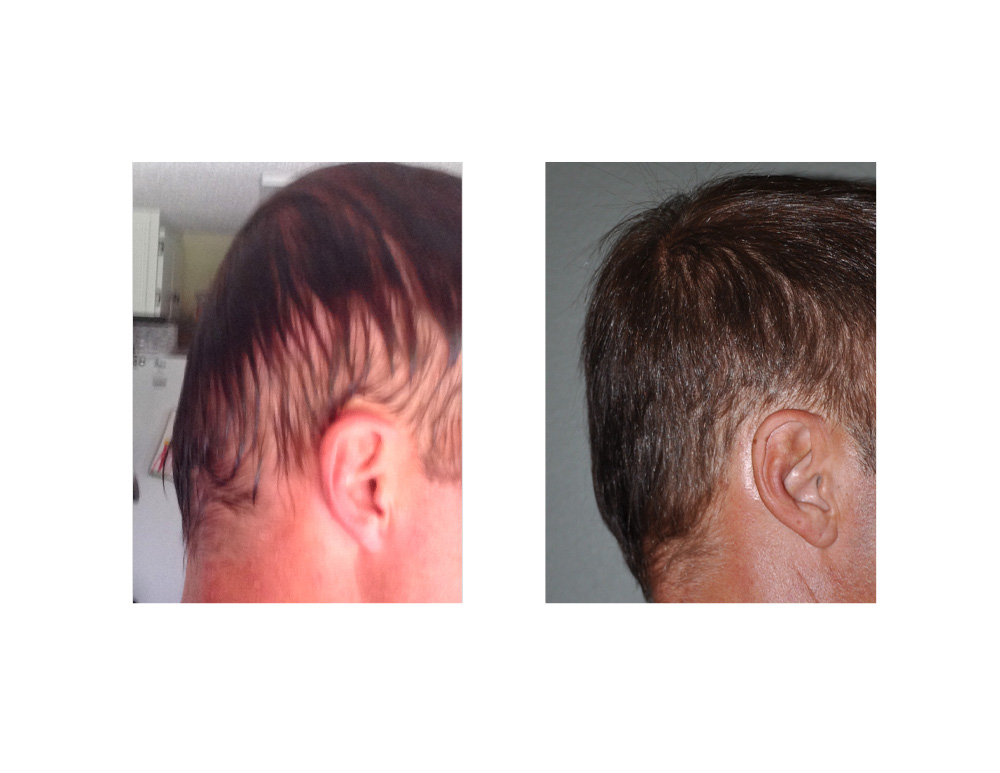 It could be seen immediately after surgery that the occipital contour was augmented to a perfectly normal shape from the profile view.
It could be seen immediately after surgery that the occipital contour was augmented to a perfectly normal shape from the profile view.
Occipital augmentation for a flat back of the head can be done using a custom implant even in a patient with prior scalp surgery such as a hair transplant. The loss of scalp tissue does require a prior scalp expansion to prevent the risk of skin necrosis over an implant or to even get the right sizes implant in place.
Case Highlights:
1) Augmentation of a flat back of the head that has had prior tissue excised and scars from hair transplants lacks adequate scalp tissue to safely cover an implant.
2) The scalp tightness caused by previous hair transplant harvests can be overcome through a first stage tissue expansion.
3) A custom occipital implant (2nd stage) can be inserted through a hair transplant harvest scar after initial scalp expansion. (1st stage)
Dr. Barry Eppley
Indianapolis, Indiana