

Background: The skull is a unique collection of bones (plates) that are interconnected and developmentally affect each other. The most common example of his relationship is that of the congenital condition known as craniosynostosis. When a cranial suture prematurely fuses, bone growth perpendicular to the suture is impeded. Thus in sagittal craniosynostosis, for example, the skull becomes long and narrow as transverse bone growth is impeded.
While not as dramatic, microforms of sagittal craniosynostosis will show similar but smaller areas of surrounding bone deficiencies. These are manifest as skull indentations around the original sagittal suture and back around its back edge at the site of the original posterior fontanelle. In the many sagittal ridge skull reductions I have done, most of which involve the posterior aspects of the ridge in front of the posterior fontanelle, show this pattern of bone indentations.
When evaluating a patient for a sagittal ridge reduction it is important to determine the contour of the surrounding bone. This is important as one has to determine if the sagittal ridge can be satisfactorily reduced to the level of the surrounding bone to give a nice rounded skull shape. Or does the surrounding bone need to be built up to meet the level of the maximal reduced ridge to get the desired shape?
Case Study: This 26 year-old male had a previous history of a high posterior sagittal ridge that was effectively burred down. This procedure was done through an existing small sagittal scar that was present from a prior biopsy of the area by prevjous doctors. The sagittal ridge had been burred down as much as possible and he was initially happy with the result. Over time he subsequently decided to build the surrounding bone as well.
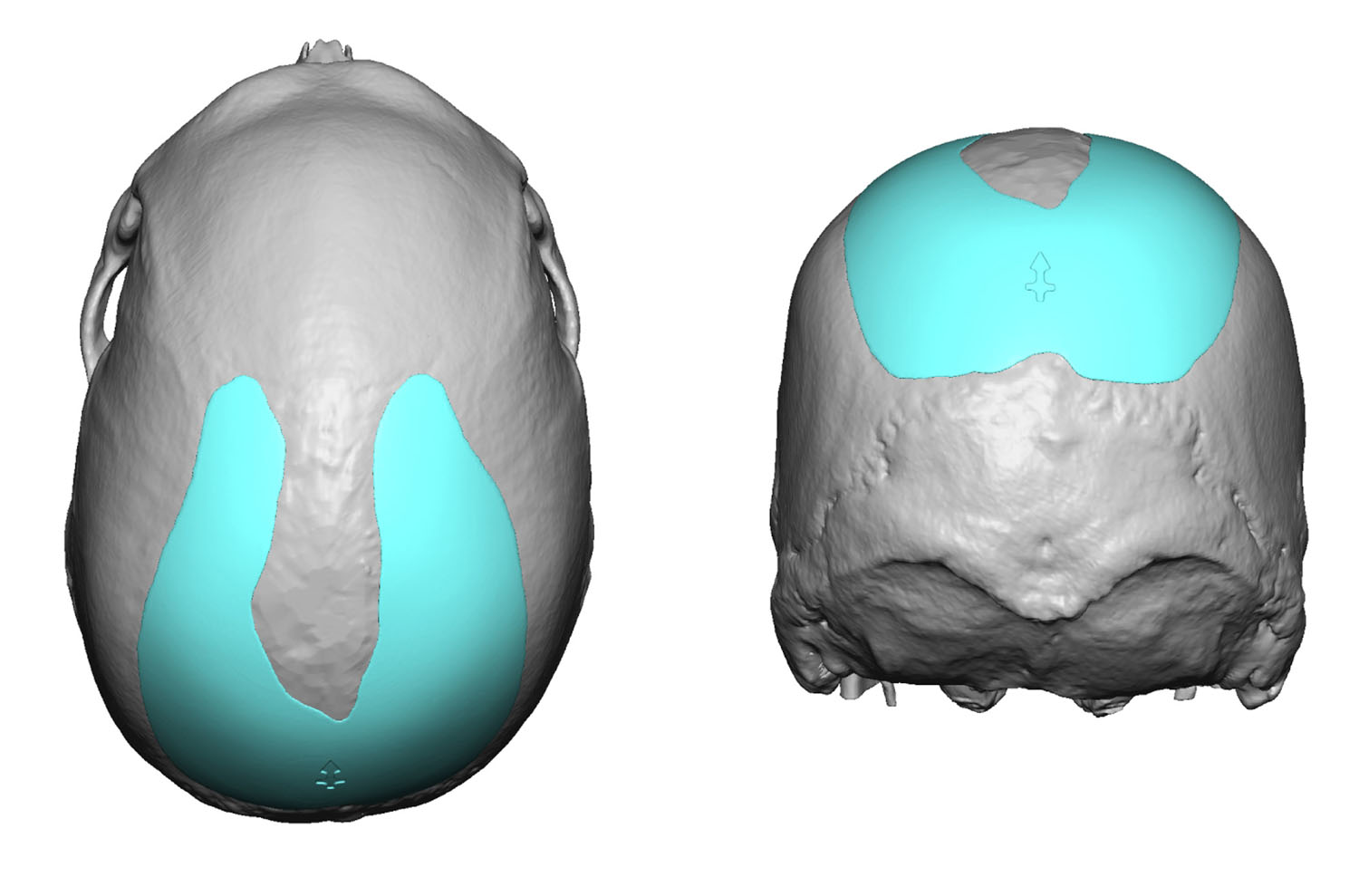
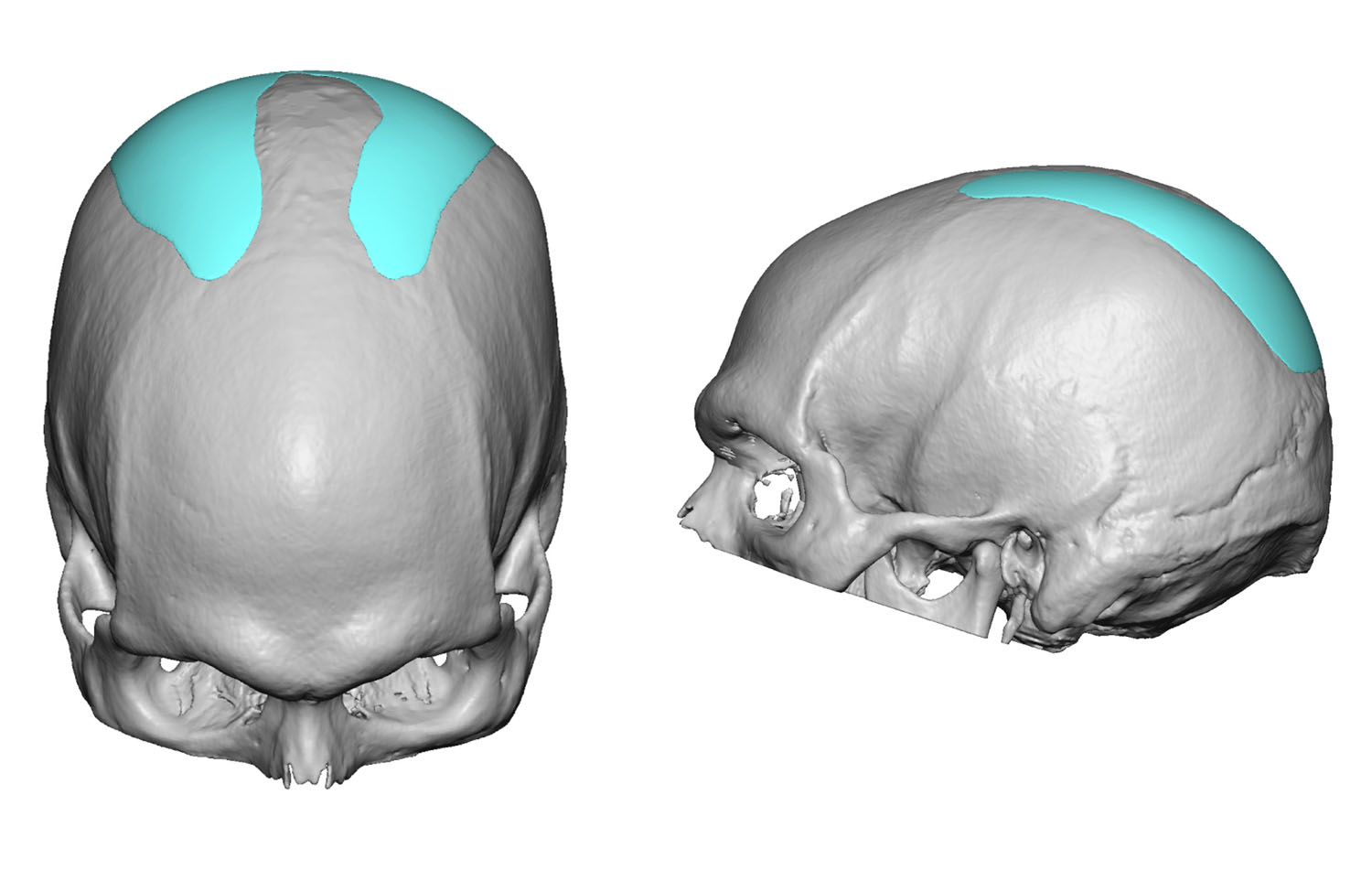 Utilizing a 3D CT scan a custom skull implant was designed to fill in the parallel parasagittal contour defects as well as cover over the depressed indentation at the back end of the original sagittal ridge. (the original posterior fontanelle) The custom skull implant had a U-shape and was fairly thin.
Utilizing a 3D CT scan a custom skull implant was designed to fill in the parallel parasagittal contour defects as well as cover over the depressed indentation at the back end of the original sagittal ridge. (the original posterior fontanelle) The custom skull implant had a U-shape and was fairly thin.
 Under general anesthesia the custom skull implant had multiple 4mm perfusion holes placed through it. It was then inserted in a folded fashion though the original small sagittal scalp incision. Once under the scalp the implant was unfolded and positioned as designed. Two small micro crews were placed to prevent any potential of any implants shifting.
Under general anesthesia the custom skull implant had multiple 4mm perfusion holes placed through it. It was then inserted in a folded fashion though the original small sagittal scalp incision. Once under the scalp the implant was unfolded and positioned as designed. Two small micro crews were placed to prevent any potential of any implants shifting.
The custom occipital-parasagittal skull implant can be a good aesthetic adjunct in the sagittal ridge reduction patient. It can be placed at the same time as the reduction or can be done secondarily if the patient is uncertain as to its contour benefit.
Highlights:
- A prominent sagittal ridge often is accompanied by a surrounding upper occipital-parasagittal skull deficiency.
- A. custom occipital-parasagittal skull implant can fill in the skull deficiency at the time of or after a sagittal ridge skull reduction.
- Such a custom skull implant can be inserted through the same small incision used for sagittal ridge reductions.
Dr. Barry Eppley
Indianapolis, Indiana